Oh, Lee, Kim, Kim, and Lyu: Social Adjustment of Adolescent Cancer Survivors: A Concept Analysis
Abstract
Purpose
This study aimed to identify the attributes of social adjustment among adolescent cancer survivors using concept analysis and to propose a definition of the concept.
Methods
In accordance with the hybrid model of concept analysis, this study employed a three-phase circular process comprising theoretical, fieldwork, and final analysis phases. A thorough literature review was conducted using MEDLINE, Embase, and Korean databases, followed by qualitative fieldwork with seven participants. The results derived from the theoretical and fieldwork phases were integrated into the final analysis phase.
Results
Four attributes of social adjustment were found in adolescent cancer survivors: having harmonious relationships with friends, having harmonious relationships with boy/girlfriends, fulfilling their present roles, and planning for and expecting future roles. The following definition of social adjustment of adolescent cancer survivors is proposed: “the conquering of difficulties arising from the continuum of childhood cancer and the achievement of the developmental tasks of typical adolescents.”
Conclusion
Social adjustment of childhood cancer survivors is crucial for integrating them into society. The findings of this study provide a basis for developing an instrument to measure the social adjustment of adolescent cancer survivors and for developing of interventions that target this group.
Key words: Social adjustment; Cancer survivors; Adolescent
INTRODUCTION
1. Need for Study
Each year, an average of 1,160 children are newly diagnosed with childhood cancer in Korea, but the 5-year survival rate has improved to 78.2%[ 1]. Although treatment methods continue to be developed, many children still experience short- and long-term complications both due to the disease itself and resulting from the intensive treatments that they receive [ 2]. Survivors of childhood cancer often report late physical effects, such as fatigue and pain, and late psychological effects, such as depression and anxiety. These late effects may negatively affect survivors’ social relationships and role performance [ 3, 4]. In general, social adjustment is defined as achieving developmentally appropriate goals in terms of relationships and roles [ 5]. Adolescent cancer survivors may experience difficulties in completing developmental tasks because of frequent hospitalizations and the need to undergo cancer treatments for relatively long periods. Survivors may also experience difficulties in developing friendships and romantic relationships [ 6, 7], as well as educational difficulties, which include failing to complete the regular school curricula, requiring special education [ 8], and obtaining less-than-optimal employment status after transitioning from a school setting [ 2]. These social adjustment problems worsen over time and negatively affect survivors’ long-term quality of life [ 9]. Nonetheless, some studies have reported positive social adjustment among adolescent cancer survivors. In these studies, no significant difference was identified between childhood cancer survivors and healthy controls in employment or marriage outcomes [ 10], and childhood cancer survivors tried to achieve their future goals through cognitive reconstruction, seeking the meaning of survival after treatment [ 11]. Despite the importance of social adjustment for adolescent cancer survivors, prior studies have reported inconsistent results; this is in part due to the absence of clear conceptual definitions [ 9]. Most quantitative studies measure social adjustment using social outcomes such as education level, employment status, and marital status [ 2]. However, since adolescents’ developmental tasks are related to the process of achieving these social outcomes (for example, adolescents are in the process of completing their education to achieve the corresponding social outcomes), it is illogical to define social adjustment as the achievement of fragmented social outcomes. Another measure of social adjustment is the social function subscale of the quality of life index, which measures social well-being [ 12]. This measure is limited in that it focuses only on friendship and does not cover the developmental tasks of adolescents. Qualitative studies have explored the process through which adolescents achieve developmental tasks while undergoing nearly unbearable treatment processes as childhood cancer patients [ 13]. However, no studies have yet identified attributes of social adjustment that reflect the experience of childhood cancer treatment and survivorship. In the United States, the Survivorship Treatment Access and Research (STAR) Act was established in 2018 to support research into the late effects of childhood cancer, including studies on care, quality of life, survivorship, and caregiver support [ 14]. In other words, the focus has shifted from the nursing care of hospitalized childhood cancer patients to caring for these patients in their life after treatment. For adolescent cancer survivors to integrate into society and maintain a high quality of life, the concept of social adjustment unique to this group is important, and an appropriate definition of this concept must be established in order to provide them with effective care. The purpose of this study was to identify the attributes of the social adjustment of adolescent cancer survivors using a hybrid model concept analysis and to propose a definition of the concept. This study provides meaningful insight into the social adjustment of childhood cancer survivors and ways of developing an instrument to assess their social adjustment.
2. Definition of Terms
1) Adolescent cancer survivors
From a biological point of view, adolescence is often defined as the period of puberty (from ages 10 to 19). However, a recent study showed that the beginning of adulthood should be defined with consideration of the timing of role transitions, including completion of education, marriage, and parenthood; thus, adolescence could be regarded as extending until the age of 24 [ 15]. Similarly, the United Nations definition of adolescence is one’s transition from a dependent child to an independent adult, which occurs between 15 and 24 years of age [ 16]. Especially for childhood cancer patients, it is better to define adolescence from a social perspective than from a traditional biological perspective, because disease and treatment often delay their timeline for fulfilling the roles they might perform as adolescents. Therefore, adolescent cancer survivors in this study were defined as adolescents aged 15~24 years who had received follow-up care for more than 6 months after the end of childhood cancer treatment.
METHODS
1. Study Design
This study used concept analysis methodology to explore and identify the attributes and characteristics of the social adjustment of adolescent cancer survivors using the hybrid model. The hybrid model of concept analysis consists of three phases: theoretical, fieldwork, and final analysis [ 17], which are described below.
2. Phase 1: Theoretical Phase
The final outcome of the theoretical phase is an operational definition of the concept of interest, based on a comparative analysis of the definitions and attributes from dictionaries and a literature review [ 17]. To explore the conceptual definitions and attributes of the “social adjustment of adolescent cancer survivors”, both the dictionary meanings and literature published in English and Korean were searched and reviewed. In addition to literature from the field of nursing, the literature reviewed in this phase included research from the fields of medicine, psychology, and sociology to include a comprehensive range of attributes and characteristics used in the social sciences. During the literature review, we searched the literature broadly, without limitations on the type of research. Since social adjustment has often been used interchangeably with the concepts of social outcome, social well-being, and social functioning in the literature, those terms were also used as keywords in this study. Other keywords that we searched for included “adolescent”, “teenage”, “pediatric”, “childhood”, “neoplasm”, “cancer”, and “survivor”. The electronic search was conducted using Ovid-MEDLINE, Ovid-Embase, KoreaMED, the Research Information Sharing Service (riss4u), and the Korean Studies Information Service System (KISS). The search was limited to publications between 2000 and June 2017.
The inclusion criteria for publications in the literature review were: reviews, qualitative and quantitative research that defined the social adjustment of childhood cancer survivors (studies using the words “social adjustment” or “social adaptation”), literature published in English or Korean, and peer-reviewed studies. Although we were interested in exploring the social adjustment of adolescents aged between 15 and 24 in this study, few studies were initially found that involved subjects in this age group, so we looked for studies including samples that overlapped with the age range 15~24 (e.g., a sample with age range from 3~15 was judged eligible, but one that included a range of 3~7 years was not) [ 18]. This age restriction did not apply to review articles. Among the final selected studies, one study was conducted on 27- to 53-year-olds. However, since it was a qualitative study on the educational trajectory of cancer survivors, and included the experiences of adolescents, we selected it for inclusion.
3. Phase 2: Fieldwork
1) Participants
In the fieldwork phase, the attributes and characteristics of social adjustment determined in the previous phase were validated and confirmed by adolescent cancer survivors.
Before participants were recruited, the study was approved by the Institutional Review Board (IRB No. 4-2017-0141). The specific inclusion criteria of participants were: being an adolescent between 15 and 24 years, being aware of one’s diagnosis, being in the post-treatment phase for at least 6 months, and not currently being treated for psychiatric problems. Recruitment was conducted at the outpatient clinic of a university hospital located in Seoul, Korea. Recruitment posters were placed in the pediatric cancer outpatient clinic. The posters contained detailed information about the primary researcher for use by individuals who felt that they would qualify for the study. In addition, we contacted information-rich participants who were recommended by a nurse (i.e., those who had returned to society after being treated for childhood cancer and could describe their experiences in detail).
Eight adolescents volunteered to participate in the study. However, one did not meet the inclusion criteria, and was therefore excluded from the study, leaving the total number of participants at seven.
2) Procedure
Prior to the interviews, the parents of children younger than 19 years of age signed a parental consent form after the researcher explained that participation in the study was voluntary and that the interview would be recorded. The participants were then informed about the purpose of the study in detail, after which they signed a written consent form and completed a background questionnaire on their demographic information (e.g., gender, age, diagnosis, treatment, age at diagnosis, time since treatment).
Semi-structured interviews were conducted face-to-face for 30 to 70 minutes. One interview was conducted per participant. For participants’ comfort and confidentiality, interviews were conducted in the consultation room, an independent space in the outpatient clinic. The interviews were audio-recorded, and participants’ non-verbal behavior during the interviews was recorded in a field notebook by a research facilitator (principal investigator, PI). Each interview began with introductory questions such as “please tell me how you have been doing in the last 3 months” and “please tell me about your typical day”. The behavior-over-time graphing method was used to minimize the potential bias of the attributes derived from the theoretical phase on the fieldwork phase. The participants were encouraged to reflect on their physical, psychological, and social adjustment since the time before diagnosis. As an example, one participant explained the graph as follows: “After treatment, I want to go out a little bit, and I’m stamping my feet, saying that I want to get out of this room. It means spending time with my friends, adjusting to my social life, and acting exactly like a typical person”( Figure 1). The researcher then asked specific, unbiased questions in response to the participant’s initial replies. Through this process, it was possible to naturally derive participants’ understanding of the meaning of social adjustment, and the attributes derived from the theoretical phase could not act as a bias in the fieldwork phase. The main questions asked during the interviews were “please tell me about the experiences or feelings you had at school or in society after you completed cancer treatment” and “what does social adjustment after cancer treatment mean to you?” As the facilitator summarized the interview responses, participants were asked to write down the three components of social adjustment that they considered the most important. Through this process, we were able to organize the interviews and ascertain whether there was anything about which these participants wanted to elaborate. The interviews were transcribed verbatim immediately after the process, and data analysis was performed simultaneously. In this qualitative study, no new themes or statements emerged after five individual interviews, at which point data saturation was reached.
3) Analysis
The PI continuously performed comparative analyses of the interviews to extract major attributes and themes. In particular, the data were coded for recurring themes using Waltz, Stickland, and Lenz’s [ 19] content analysis method. For this process, the transcripts were read multiple times, significant statements were extracted from the narrative content, extracted statements were assigned to a theme, and major attributes were derived from themes that were grouped together and abstracted. Data analysis was performed independently by the PI and one experienced nurse (who is not a co-author of the study, is able to analyze concepts without bias, has a doctoral degree, and is experienced in qualitative research on childhood cancer survivors), who discussed the results of the analysis together to reach a consensus.
4. Phase 3: Final Analysis
In the final analysis phase, the findings from both the theoretical and fieldwork phases were analyzed comparatively and integrated to arrive at a conceptual definition [ 17]. The data obtained during the theoretical and fieldwork phases of the study were then compared and analyzed, the attributes were extracted, and the concept of social adjustment of adolescent cancer survivors was defined based on the findings. The findings were double-checked by assessing content validity, which was evaluated by six experts consisting of a professor of nursing, an experienced nurse manager of a pediatric oncology ward, a pediatric hematology coordinator, a nurse with over 10 years of experience working with childhood cancer patients, a pediatric hematologist, and a mother of an adolescent cancer survivor.
RESULTS
1. Phase 1: Theoretical Process
1) Dictionary meaning of “social adjustment”
Social adjustment refers to the “adaptation of the person to the social environment. Adjustment may take place by adapting the self to the environment or by changing the environment”[ 20].
2) Attributes of social adjustment of adolescent cancer survivors from the literature review
A total of 1,770 articles were found from the database search, and two more studies were added after a manual search. Finally, 10 studies were selected to review the meaning of social adjustment of survivors of childhood cancer. The design of the included studies ranged from reviews, quantitative research, and qualitative research. Table 1 presents a summary of these 10 studies. In the theoretical phase, social adjustment of adolescent cancer survivors was determined to refer to achievement of the same developmental stage as that of their peers [A1-A4]. Nursing studies that explored social adjustment among childhood cancer patients commonly used qualitative rather than quantitative methodologies [A2,A3,A5], focusing on their process of accomplishing developmental tasks, such as maintaining friendships and academic performance, while experiencing nearly unbearable treatments for cancer.
After treatment for childhood cancer, adolescents experience difficulties in establishing harmonious relationships with friends, as prior friendships could have been discontinued because of the cancer diagnosis and treatment regimen [A1,A2,A4]. For cancer patients, having harmonious relationships with friends means being accepted and supported by friends and getting along with them [A3], feeling that they are not different from their friends [A3,A5], not being socially isolated, and being involved in activities [A6].
Establishing romantic relationships is an important developmental task during adolescence, but after childhood cancer treatment, adolescents have difficulties in developing and maintaining such relationships because of changes in their appearance and/or negative attitudes towards people who have been diagnosed with cancer [A4,A7].
A secondary role that must be fulfilled during adolescence is academic performance, which fosters the development of intellectual functioning. However, those who have completed childhood cancer treatments may fall behind compared to their peers. This may result in a loss of confidence when they return to school after intensive cancer treatment, and they may not consider academic performance as a priority in their lives. Many studies have reported educational achievement to be an attribute of social adjustment, including continuing with school [A5,A6,A8-A10], not requiring special education [A6,A9], and not falling behind in academic performance [A5,A6].
In adults, social achievements such as occupation, marriage, independence, and parenthood can be viewed as indicators of social adjustment [A4,A8,A9], but for adolescents, social adjustment involves preparing for these goals. Three studies proposed certainty about future plans as an attribute of social adjustment of adolescent cancer survivors [A4,A8,A10].
In summary, the following four attributes were identified: having harmonious relationships with friends, having harmonious relationships with boy/girlfriends, academic performance, and planning for future roles (occupation, independence, marriage, and parenthood). The social adjustment of adolescent cancer survivors was tentatively defined as follows: “After returning to normal life after the treatment of childhood cancer, the survivor adjusts to the changed environment, maintains a harmonious relationship with friends and boy/girlfriends, continues with studies, and plans for future roles.”
2. Phase 2: Fieldwork
1) Characteristics of participants
The participants were five females (71.4%) and two males (28.6%). The mean age of the seven participants was 18.1 years (range: 15~21), and their mean age at the time of treatment completion was 15 (range: 9~19). The mean post-treatment period was 3 years (range: 6 months~8 years 11 months). Five participants had been diagnosed with leukemia (71.4%), one with lymphoma, and one with osteosarcoma. All leukemia and lymphoma patients had received chemotherapy and transplantation, and the osteosarcoma patient had received chemotherapy and surgery. Three were either on a leaves of absence from school or continued their education through an online school.
2) Attributes of social adjustment in adolescent cancer survivors
The content analysis in the fieldwork revealed the following attributes: having harmonious relationships with friends, having harmonious relationships with boy/girlfriends, fulfilling their present roles, finding a dream job, becoming independent (managing without parental help), and expecting marriage and childbearing ( Table 2).
(1) Having harmonious relationships with friends
Explaining the meaning of social adjustment after cancer treatment, many participants stated that social adjustment was related to relationships with friends. The most important component of social adjustment for them was a normal life in which they could spend time with friends, get along, and have fun. Survivors who had just finished treatment were still isolated and did not frequently spend time with their friends, and some participants were deeply hurt when they felt that their friends had rejected them. Participants differentiated themselves from others by referring to healthy friends as “normal people” or “typical people”. They also tried to hide their history of cancer because they were concerned that, if it became known, their friends might feel burdened and the relationship would deteriorate. Some participants said the following:
Frankly, there was a very high wall between them and me. I always felt that a wall existed between typical people and me. Whenever I saw peers, I felt that I was different, that they were different, and that I could not be like them. So I was very depressed.(Participant D, 18-year-old female) I try not to make friends. I have a wound on my stomach. I hate to touch it. I hate to say anything that hurts. If I say I’ve got cancer, I think I’ll be ostracized by my friends.(Participant G, 15-year-old male)
(2) Having harmonious relationships with boy/girlfriends
Changes in appearance, such as alopecia and lowered confidence, caused adolescent cancer survivors to intentionally avoid spending time with their boy/girlfriends. One participant cried while stating that she had not seen her boyfriend since she had been diagnosed with cancer. The experience of rejection by a boy/girlfriend due to changes in one’s appearance left a “psychological scar”. In terms of revealing one’s history of childhood cancer to their boy/girlfriends, some participants said they would not like to hide it, while others said that they avoided telling them the details. Some participants said the following:
[Do you have a boyfriend?] Yes… So, I am crying because of my hair. I am OK with my friends, but because of my boyfriend… (crying). I haven’t seen him since I was diagnosed. (Participant B, 19-year-old female) I had a boyfriend, and I was sick and my hair was falling out, so my boyfriend did not want to see me, so we broke up. After the treatment, cancer had many effects on my romantic relationships. (Participant E, 20-year-old female)
(3) Fulfilling their present roles
The greatest challenge for participants after returning to everyday life following the period of treatment was catching up with friends and not falling behind in their academic performance. Participants felt great stress from this, and some quit high school and later entered college after taking the High School Graduate Equivalency Test for Self-Study Students (the Korean equivalent of the General Educational Development [GED] test in the United States and Canada). Further, participants were excluded from school group activities, like physical education and school trips, and some stated that not taking part in such activities made them feel like they were walking on eggshells. One participant said the following:
After a year’s break from studying, I did not remember anything. It was really difficult. Now, I am trying not to be overambitious, and just trying to do… trying to take it as is. I am trying really hard not to stress out, but there still is a lot of stress …. I never went to physical education class, and the teacher gave me a very low grade. (Participant E, 20-year-old female)
(4) Finding a dream job
Cancer altered the participants’ career paths, which was a positive experience for some and a negative experience for others. Participants attempted to identify their skills and achieve their dreams under those circumstances. They said that they felt like “a normal person” when they were learning what they liked and trying out those possibilities. Participants were also concerned about whether revealing their history of cancer would work positively for them in their future career search. Since serving in the military is a compulsory duty for men in South Korea, when applying for a job, male participants were compelled to make their history of cancer public when indicating why they have not fulfilled their duty of military service. Although the participants were worried about this situation, they were aware that, ultimately, their history of cancer could not be hidden and were trying to use it positively. A female participant said the following:
In self-introductory statements in job applications, you are expected to write why you are applying for the job or why you became a nurse, and I can only write about my experience of being sick. When I didn't get selected at the application screening stage, a friend of mine was selected although we had the same qualifications. When it happened, even my mom asked me whether it was because I wrote about it [my history of cancer]. And so I thought about whether my illness worked as a minus…. If I don't talk about it, I have nothing else to say when they ask me why I want to be a nurse. (Participant F, 21-year-old female)
(5) Becoming independent without their parents' help
Although the participants were dependent on their parents during treatment, they recognized the need to function independently among those who would not accept them unconditionally. They said that although becoming independent from their parents was scary, it would be necessary for them to be a “typical adult”. One participant said the following:
Right now, my mom accepts my petulance and everything because undergoing cancer treatment is hard, and the adults always accept it when I tell them I'm having a hard time. But when I return to society, people will not know that I was sick. So, I’ll have to do things not at my convenience. Even if it is not convenient, I will take it as it is. (Participant A, 18-year-old female)
(6) Expecting marriage and childbearing
Some participants had negative perceptions of, or felt insecure about, marriage and childbearing. They protected their feelings by not anticipating the future task of childbearing. However, some participants said that they would consider alternatives, like in-vitro fertilization (IVF), while others were expectant about the prospect, and said that it would be fine as long as they met a person who could understand them. One participant said:
I will never be able to have children. I heard it 6 months ago…. I sometimes think that I would like to remain single. Because I don't have expectations. I don't get my hopes up about the future, because I’ll be more hurt if I have expectations. So, I give up because I cannot attain anything. I tend to just focus on other daily activities. I watch TV dramas where a woman is scolded by her mother-in-law and accused of discontinuing the family lineage because she cannot have a baby. Such dramas make me not want to get married even more…. (Participant D, 18-year-old female) I've heard that chemotherapy reduces ovarian function. My friends and I continue to go to obstetrics and gynecology for cancer treatment. Some of my friends are told that they won't ever get pregnant, and I'm not going to get pregnant naturally. But I don't feel stressed because I have the option of IVF if I want to later. (Participant F, 21-year-old female)
3. Phase 3: Final Analysis
In the final analysis phase, the findings from the literature review and the empirical study were examined comprehensively to determine the attributes of social adjustment of adolescent cancer survivors.
Most of the attributes identified in the theoretical phase were also derived from the fieldwork phase, and attributes with similar meanings were integrated and renamed. Howver, there were some differences in the content of attributes. In the theoretical phase, only academic performance was identified, but in the fieldwork phase, participation in group activities such as sports competitions and school trips was added, for which reason this concept was revised to “fulfilling their present roles”. In addition, planning for future roles was derived from attributes in the theoretical phase, but in the fieldwork phase, the topic of expecting roles in addition to planning for future roles was added, yielding “planning for and expecting future roles”. Ultimately, four main attributes were identified in this study: having harmonious relationships with friends, having harmonious relationships with boy/girlfriends, fulfilling their present roles, and planning for and expecting future roles ( Table 3). Based on all the three phases discussed above, the following definition of social adjustment of adolescent cancer survivors is proposed: “the conquering of difficulties arising from the continuum of childhood cancer and the achievement of the developmental tasks of typical adolescents, such as having harmonious relationships with friends, having harmonious relationships with boy/girlfriends, fulfilling their present roles, and planning for and expecting future roles.”
DISCUSSION
Cancer survivors continue to struggle with physical, mental, and social challenges after cancer treatment. Through the concept analysis of social adjustment of adolescent cancer survivors, four attributes were identified: having harmonious relationships with friends, having harmonious relationships with boy/girlfriends, fulfilling their present roles, and planning for and expecting future roles. It might be hard for adolescent cancer survivors to achieve certain developmental tasks due to both the disease itself and the treatment regimen. The participants considered social adjustment to involve overcoming difficulties (such as disclosure and acceptance of their cancer diagnosis, difficulties in establishing relationships, and the feeling of lagging behind in achieving developmental tasks) and achieving the same developmental tasks as their friends with typical health. In other words, they struggled within the continuum of childhood cancer with the aim of achieving the same developmental tasks as their friends to feel normal. This finding is similar to that of Ramini, Brown, and Buckner’s [ 21] work discussing the adaptive strategies of adolescents with cancer. All of the adolescents with cancer in their study wanted to feel normal. One of the participants rejected home schooling and completed a formal education course in order to achieve the same developmental stage as his/her friends. Similarly, the childhood cancer survivors (aged 19 to 31) who participated in the study by Tsonis et al. [ 22] felt that they were different from their friends because they could not participate in activities with them. In addition, learning difficulties made it more difficult for them to reintegrate into peer groups. The pursuit of normality is a characteristic theme in the post-treatment adjustment of childhood cancer patients, but no research has described it in relation to social adjustment. The first attribute identified in the present study was “having harmonious relationships with friends”. Participants differentiated themselves from their healthy friends by referring to them as “normal people” and “typical people”, sensed “a wall between typical people” and themselves, and often felt frustrated with situations in which they could not have harmonious relationships with others, but felt distant and alone. It is a “traumatic social experience” for childhood cancer survivors to experience a feeling of being different, excluded, picked on, or bullied [ 23]. Such experiences can remain painful throughout life and require special attention [ 23]. Particularly noteworthy in these social relations was the disclosure of one’s cancer history. This is similar to the results of previous studies, which reported that survivors tended to hide their history of childhood cancer in order to avoid negative recognition or discrimination from others [ 3]. Advocacy campaigns provided more opportunities for survivors to grow positively, but the advocacy activities for childhood cancer survivors in Korea are insufficient [ 24]. In order to reduce social prejudices against childhood cancer patients, we suggest creating an intervention protocol that is self-sufficient and uses the community as a tool. For example, interventions might include strategies to transform a community into a safe space to disclose sensitive information. The second attribute identified herein was “having harmonious relationships with boy/girlfriends”. Many of the participants had a negative body image, which caused problems with the formation of bonds and the development of intimacy with others. Previous studies have found that changes in physical appearance and feelings of being different may have a negative effect on the development of intimate relationships. In addition, childhood cancer survivors had few opportunities to exchange sexual information with friends, and parental overprotection was also found to be a factor influencing romantic relationships [ 25]. The role of oncology nurses in Korea is diverse and includes physical examinations, responding to advice from medical personnel, cooperation and coordination with other departments, research, and self-help management. Patients are also more comfortable with nurses than with doctors, so we expect nurses to play a role in counseling, education, and meeting the psychosocial needs of patients and their families. Therefore, oncology nurses may be able to encourage survivors to develop healthy romantic relationships or, in some cases, ask psychologists to cooperate to this end. In addition, nurses can also help survivors develop a positive body image and confidence by suggesting the use of props such as wigs and hats. “Fulfilling their present roles” was the most frequently mentioned theme in the fieldwork phase. Childhood cancer can result in low academic achievement and dropping out of school. Most participants in this study had difficulties with academic achievement due to the interruption of their studies during illness and treatment and the disabilities caused by treatment toxicity. In the United States, the Individuals with Disabilities Education Act (IDEA) gives special education rights to patients with chronic illnesses [ 26]. In Korea, childhood cancer is classified as a health disability on the basis of the Special Education Law for Persons with Disabilities enacted in 2005, and receiving education through a hospital-based school or online class is considered regular attendance [ 3]. Since Korean hospital-based schools and online classes target all health-impaired students without distinguishing among diseases, it is difficult to provide individualized education that reflects the characteristics of childhood cancer. Additional problems may occur if actual education is not conducted due to childhood cancer patients’ poor attendance and low motivation [ 27]. Therefore, it is necessary to improve the quality of education provided to children and adolescents with cancer and to provide personalized education to those who are experiencing various medical conditions so that they can fulfill the corresponding education standards, rather than simply meeting attendance requirements. “Planning for and expecting future roles” refers to identifying one’s skills and making efforts to achieve one’s dreams, as well as preparing for and expecting independence, marriage, and childbearing. Adolescent cancer survivors may search for career paths but feel that they are lagging behind in their professional track and fear a situation wherein they may have to change their occupational goals because of cancer [ 28]. Participants were deeply concerned about the possibility of having to change their career path because of cancer and recognized the significance of planning and preparing for their future roles as factors in social adjustment, despite various difficulties. Nonetheless, in some cases, the experience of childhood cancer allowed participants to realize their aptitude; one participant said, “My dream is to become a cartoonist. It was nice to have more time to draw pictures while I was being treated. I want to show my experiences in the hospital in the form of a cartoon.” Because the adjustment of childhood cancer survivors should be considered while they receive post-diagnosis treatment, not after treatment [ 21], nurses can continuously support patients to make positive social adjustments by planning for their future during treatment. With regard to marriage and pregnancy, some of the participants protected their emotions by not expecting such life events. Many childhood cancer survivors are uncertain about their reproductive capacity. However, many are also reluctant to give up on having children, and therefore consider the possibility of adopting or marrying people who already have children [ 29]. Marriage and pregnancy-related issues may not yet be a primary concern when childhood cancer patients are first diagnosed; however, participants said they felt scared and frustrated about their reproductive capacity when they were informed of the possible effects of treatment on their fertility before treatment began [ 30]. Thus, nurses may be able to support childhood cancer patients receiving treatment by having an open dialogue on these issues and by discussing various options for fertility preservation. In this study, the social adjustment of adolescent cancer survivors was shown to be a multi-dimensional concept consisting of four attributes. However, most quantitative studies conducted so far have simply measured adolescent cancer survivors’ social adjustment through their achievement of social outcomes. Therefore, we recommend that an instrument be developed to measure the multidimensional aspect of social adjustment, considering the developmental tasks of adolescent cancer survivors. The results of this study could be used to develop tools for measuring the social adjustment of adolescent cancer survivors. This study was limited to patients who received follow-up at a single hospital. Therefore, their experiences might not be generalizable as representative of the experiences of all adolescent cancer survivors. However, this study is significant in that it is the first to propose a conceptual definition of the social adjustment of adolescent cancer survivors in South Korea. As the definition of social adjustment is likely to vary across developmental stages, further comparative research is needed to analyze the concept of social adjustment for children and adult survivors.
CONCLUSION
The characteristics discussed above should be considered in research on adolescent cancer survivors because they face difficulties in achieving developmental goals within the continuum of disease. Ultimately, the social adjustment of childhood cancer survivors is crucial for their integration into society. No prior study to date has defined the concept of the social adjustment of adolescent cancer survivors. In this study, four attributes were derived by analyzing the concept of the social adjustment of adolescent cancer survivors using a hybrid model. The results of this study can be used as a basis for developing an instrument to measure the social adjustment of adolescent cancer survivors, and the results may also contribute to the development of interventions for adolescent cancer survivors in the future by helping nurses and researchers understand the difficulties that survivors encounter.
REFERENCES
1. Park HJ, Moon EK, Yoon JY, Oh CM, Jung KW, Park BK, et al. Incidence and survival of childhood cancer in Korea. Cancer Research and Treatment. 2016;48(3):869-882. https://doi.org/10.4143/crt.2015.290
  2. Prasad PK, Hardy KK, Zhang N, Edelstein K, Srivastava D, Zeltzer L, et al. Psychosocial and neurocognitive outcomes in adult survivors of adolescent and early young adult cancer: A report from the childhood cancer survivor study. Journal of Clinical Oncology. 2015;33(23):2545-2552. https://doi.org/10.1200/JCO.2014.57.7528
3. Nam SI, Choi KH. School reintegration, adjustment difficulties, and services for childhood cancer survivors. Korean Journal of Social Welfare Research. 2013;38:181-215.
4. Hauken MA, Holsen I, Fismen E, Larsen TM. Participating in life again: A mixed-method study on a goal-orientated rehabilitation program for young adult cancer survivors. Cancer Nursing. 2014;37(4):E48-E59. https://doi.org/10.1097/NCC.0b013e31829a9add
5. Hocking MC, McCurdy M, Turner E, Kazak AE, Noll RB, Phillips P, et al. Social competence in pediatric brain tumor survivors: Application of a model from social neuroscience and developmental psychology. Pediatric Blood and Cancer. 2015;62(3):375-384. https://doi.org/10.1002/pbc.25300
6. Boydell KM, Stasiulis E, Greenberg M, Greenberg C, Spiegler B. I'll show them: The social construction of(in)competence in survivors of childhood brain tumors. Journal of Pediatric Oncology Nursing. 2008;25(3):164-174. https://doi.org/10.1177/1043454208315547
7. Thompson AL, Marsland AL, Marshal MP, Tersak JM. Romantic relationships of emerging adult survivors of childhood cancer. Psycho-Oncology. 2009;18(7):767-774. https://doi.org/10.1002/pon.1471
8. Ness KK, Bhatia S, Baker KS, Francisco L, Carter A, Forman SJ, et al. Performance limitations and participation restrictions among childhood cancer survivors treated with hematopoietic stem cell transplantation: The bone marrow transplant survivor study. Archives of Pediatrics and Adolescent Medicine. 2005;159(8):706-713. https://doi.org/10.1001/archpedi.159.8.706
9. Schulte F, Brinkman TM, Li C, Fay-McClymont T, Srivastava DK, Ness KK, et al. Social adjustment in adolescent survivors of pediatric central nervous system tumors: A report from the childhood cancer survivor study. Cancer. 2018;124(17):3596-3608. https://doi.org/10.1002/cncr.31593
10. Mader L, Vetsch J, Christen S, Baenziger J, Roser K, Dehler S, et al. Education, employment and marriage in long-term survivors of teenage and young adult cancer compared with healthy controls. Swiss Medical Weekly. 2017;147:w14419. https://doi.org/10.4414/smw.2017.14419
17. Schwartz-Barcott D, Kim HS. An expansion and elaboration of the hybrid model of concept development In: Rodgers BL, Knafl KA, editors. Concept development in nursing: Foundations, techniques, and applications. 2nd ed. Philadelphia: W.B. Saunders Company; 2000. p. 129-159.
18. Hanratty J, Livingstone N, Robalino S, Terwee CB, Glod M, Oono IP, et al. Systematic review of the measurement properties of tools used to measure behaviour problems in young children with autism. PLoS One. 2015;10(12):e0144649. https://doi.org/10.1371/journal.pone.0144649
19. Waltz CF, Strickland OL, Lenz ER. Measurement in nursing and health research. 4th ed. New York: Springer Publishing Company; 2010. p. 279-285.
20. Campbell RJ. Campbell's psychiatric dictionary. 9th ed. New York: Oxford University Press; 2009. p 18.
21. Ramini SK, Brown R, Buckner EB. Embracing changes: Adaptation by adolescents with cancer. Pediatric Nursing. 2008;34(1):72-79.
22. Tsonis M, McDougall J, Mandich A, Irwin J. Interrelated processes toward quality of life in survivors of childhood cancer: A grounded theory. The Qualitative Report. 2012;17(45):1-18.
23. Howard AF, Tan de Bibiana J, Smillie K, Goddard K, Pritchard S, Olson R, et al. Trajectories of social isolation in adult survivors of childhood cancer. Journal of Cancer Survivorship. 2014;8(1):80-93. https://doi.org/10.1007/s11764-013-0321-7
27. Park KO, Oh WS. Teachers' perception on difficulties and educational supports for students with health impairment in the school in hospital. Korean Council of Physical, Multiple and Health Disabilities. 2012;55(3):117-139. https://doi.org/10.20971/kcpmd.2012.55.3.117
28. Warner EL, Kent EE, Trevino KM, Parsons HM, Zebrack BJ, Kirchhoff AC. Social well-being among adolescents and young adults with cancer: A systematic review. Cancer. 2016;122(7):1029-1037. https://doi.org/10.1002/cncr.29866
30. Nieman CL, Kinahan KE, Yount SE, Rosenbloom SK, Yost KJ, Hahn EA, et al. Fertility preservation and adolescent cancer patients: Lessons from adult survivors of childhood cancer and their parents. Cancer Treatment and Research. 2007;138:201-217.
Figure. 1.
An illustration of graphs and diagrams drawn during the interview (participant D, 18-year-old female). 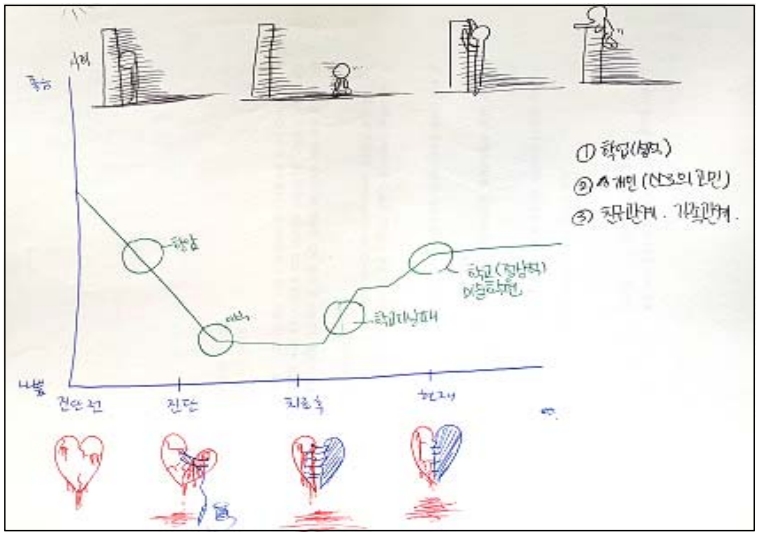
Table 1.
Summary of the Literature (N=10)
|
First author |
Year/country |
Study design |
Sample |
Key statements related to the attributes of social adjustment |
|
Eiser |
1994/UK |
Review |
Childhood cancer survivors |
Life goal achievement (relationships with friends, employment status, marriage or the ability to form a close relationship, birth of healthy children, and the attainment of life insurance, academic plans, changes in career goals because of the illness) |
|
Boman |
2004/Sweden |
Cross-sectional case-control study |
Young adult survivors (aged 18 to 29) of childhood cancer (n=30), control group (n=30) |
Type of habitation, educational status, formation of own family, birth of own children, employment, leisure activities, social mobility, planning for future roles (marriage, parenthood, occupation) |
|
Punyko |
2007/USA |
Cross-sectional case-control study |
Survivors of childhood rhabdomyosarcoma (aged≥18) (n=417), siblings (n=2,685) |
Completed high school, special education, entered the workforce, number of sick days, having been married |
|
Chen |
2008/Taiwan |
Qualitative study |
Adolescent and young adult survivors (aged 13 to 22) (n=7) |
Interpersonal relationships |
|
Ramini |
2008/UK |
Qualitative study |
Adolescents with cancer (aged 16 to 25) (n=4) |
Desire to feel normal (refusal to be home-schooled in order to graduate with friends, talking with friends about school life), peer acceptance, support from friends |
|
Thompson |
2009/USA |
Cross-sectional case-control study |
Emerging adult survivors of childhood cancer (aged 18 to 25) (n=60), control group (n=60) |
Romantic relationships, including perceived relationship satisfaction |
|
Schulte |
2010/Canada |
Review |
Child and adolescent survivors of brain tumors |
Involvement in activities, social interaction patterns, school performance, social relationships, social isolation |
|
Dumas |
2015/France |
Qualitative study |
Childhood cancer survivors (aged 27 to 53) (n=76) |
Educational trajectories (cancer as a reason for school dropout and early entry into working life), choices or decisions that survivors related to the illness in the making of their career plans, cancer as an obstacle in career aspirations, resulting in an upward social trajectory |
|
Hocking |
2015/USA |
Review |
Childhood brain tumor survivors |
Others' perceptions and self-perceptions of the quality of a child's social relationships and how well they attain socially desirable and developmentally appropriate goals |
|
Son |
2011/Korea |
Qualitative study |
Adolescent cancer patients or cancer survivors (aged 16 to 21) (n=10) |
Falling behind friends |
Table 2.
Attributes and Themes in Fieldwork
|
Attributes |
Themes |
|
Having harmonious relationships with friends |
Acceptance or refusal by friends |
|
Spending time with friends face-to-face |
|
Conception of self as different from friends |
|
Engaging in the leisure activities enjoyed by friends of the same age |
|
Attitude toward disclosing their history of childhood cancer |
|
Having harmonious relationships with boy/girlfriends |
Avoiding spending time with boy/girlfriends |
|
Low confidence in spending time with boy/girlfriends |
|
Rejected by boy/girlfriends |
|
Attitude toward disclosing their history of childhood cancer |
|
Fulfilling their present roles |
Difficulty in continuing school |
|
Falling behind in school because of self-perceived weakness caused by cancer |
|
Unable to participate in group activities at school |
|
Finding a dream job |
Discovering their aptitude |
|
Trying to achieve their dreams |
|
Attitude toward disclosing their history of childhood cancer when getting a job |
|
Becoming independent without their parents' help |
Recognizing the need to become independent |
|
Confidence in becoming independent |
|
Expecting marriage and childbearing |
Negative perception of the influence of cancer on future roles |
|
Being hurt by the loss of opportunities for future roles |
|
Having no expectations about future roles |
Table 3.
Attributes of the Theoretical, Fieldwork, and Final Analysis Phases
Theoretical phase
|
Fieldwork phase
|
|
Final analysis phase
|
|
Attributes |
Attributes |
Attributes |
Definition |
|
Having harmonious relationships with friends |
Having harmonious relationships with friends |
→ |
Having harmonious relationships with friends |
Are accepted into a peer group, maintain contact with friends, engage in the leisure activities enjoyed by friends, do not feel socially isolated, do not feel that they are different from their friends, and do not withdraw from relationships because of the cancer diagnosis |
|
Having harmonious relationships with boy/girlfriends |
Having harmonious relationships with boy/girlfriends |
→ |
Having harmonious relationships with boy/girlfriends |
Have the ability to form and maintain relationships with boy/girlfriends, are confident in spending time with boy/girlfriends, are accepted by boy/girlfriends, and do not withdraw from relationships because of the cancer diagnosis |
|
Academic performance |
Fulfilling their present roles |
→ |
Fulfilling their present roles |
Do not discontinue or give up on schooling, do not fall behind their peers in academic performance, and participate in group activities at school |
|
Planning for future roles (occupation, independence, marriage, parenthood) |
Finding a dream job |
↘ |
Planning for and expecting future roles |
Identify their skills and achieve their dreams, recognize their need for independence, are confident in being independent without help from their parents, and do not perceive the influence of a cancer diagnosis on marriage and childbearing negatively or give up on hopes about them |
|
Becoming independent without their parents' help |
→ |
|
Expecting marriage and childbearing |
↗ |
Appendices
Appendix 1.
Citations of studies included in this Study
1. Hocking MC, McCurdy M, Turner E, Kazak AE, Noll RB, Phillips P, et al. Social competence in pediatric brain tumor survivors: Application of a model from social neuroscience and developmental psychology. Pediatric Blood and Cancer. 2015;62(3):375-384. https://doi.org/10.1002/pbc.25300
3. Ramini SK, Brown R, Buckner EB. Embracing changes: Adaptation by adolescents with cancer. Pediatric Nursing. 2008;34(1):72-79.
4. Eiser C, Havermans T. Long term social adjustment after treatment for childhood cancer. Archives of Disease in Childhood. 1994;70(1):66-70.
7. Thompson AL, Marsland AL, Marshal MP, Tersak JM. Romantic relationships of emerging adult survivors of childhood cancer. Psycho-Oncology. 2009;18(7):767-774. https://doi.org/10.1002/pon.1471
8. Boman KK, Bodegård G. Life after cancer in childhood: Social adjustment and educational and vocational status of young-adult survivors. Journal of Pediatric Hematology/Oncology. 2004;26(6):354-362. https://doi.org/10.1097/00043426-200406000-00005
9. Punyko JA, Gurney JG, Scott Baker K, Hayashi RJ, Hudson MM, Liu Y, et al. Physical impairment and social adaptation in adult survivors of childhood and adolescent rhabdomyosarcoma: A report from the Childhood Cancer Survivors Study. Psycho-Oncology. 2007;16(1):26-37. https://doi.org/10.1002/pon.1072
10. Dumas A, Cailbault I, Perrey C, Oberlin O, De Vathaire F, Amiel P. Educational trajectories after childhood cancer: When illness experience matters. Social Science and Medicine. 2015;135:67-74. https://doi.org/10.1016/j.socscimed.2015.04.031
|
|












