INTRODUCTION
Fathers willingly participate in their wives' pregnancy, childbirth, and child-rearing processes, and make various efforts to become better fathers. However, while raising young children, fathers sometimes feel uncomfortable and complain of alienation [1,2]. Existing parenting-related nursing intervention programs insufficiently reflect fathers' unique educational needs and questions; instead, fathers want a well-designed program that fully understands their needs and addresses their concerns [1,3,4].
As mothers' social advancement gradually increases, fathers are more actively participating in raising young children, including infants under the age of 1, than was previously the case. Fathers need support from health professionals, especially nurses, to successfully adapt to the increasing demands of their roles [2]. A study on the "father effect" showed that fathers' participation in parenting had a positive effect on children's cognitive-emotional social development [5]. However, fathers are sometimes overwhelmed with work-family balance, as they are required to adapt to role changes due to childbirth and changing relationships, as well as acquiring knowledge and skills to care for infants [6]. In particular, fathers of infants simultaneously feel burdened by and interested in caring for their children. Infancy is a period of explosive growth during which children are completely dependent on their parents. These characteristics of infancy lead fathers to feel a greater sense of responsibility and burden.
No period in life is characterized by more rapid change and growth than infancy, and growth and development during this period affect the entirety of a person’s subsequent life; therefore, infancy is a very important period. Parent-child interactions during this period contribute to the formation of attachment between the father and the child, which has a decisive influence on emotional development during infancy and later life [7]. Behavioral observation is effective for analyzing the quality of attachment relationships [8]. However, studies focusing on educational programs and interventions related to parent-child interactions and examining their effects are lacking, and most previous studies have dealt with parental participation [9]. Moreover, very few studies have examined the effectiveness of educational and intervention programs targeting fathers that fully reflect the characteristics of infancy (defined as the period between birth and 12 months of age).
According to Barnard’s child health assessment interaction theory [10], interactions occur at the environment-caregiver-child level. The three elements intersect at the father's knowledge of child-rearing, attachment to the infant, the clarity of the child's signals to the caregiver, and the child's temperament [10]. The father's sensitivity is a modifiable factor. Recent studies have confirmed that caregivers’ sensitivity could be enhanced by a parent-child interaction intervention program that provides expert advice on improving their interactive behavior based on video-recorded interactions between caregivers and children [9,11].
Therefore, the purpose of this study was to determine whether the application of a parent-child interaction promotion program developed by the first author would promote infant developmental knowledge, interaction, and attachment through a comparison between an experimental group and a control group. This study was also conducted to confirm the applicability of this program for fathers in the local community by investigating the effects of the educational intervention. The hypotheses of this study were as follows:
Hypothesis 1. The intervention will increase child-rearing knowledge compared to the control group.
Hypothesis 2. The intervention will improve father-infant interactions compared to the control group.
Hypothesis 3. The intervention will increase father-infant attachment compared to the control group.
METHODS
Ethics statement: This study was approved by the institutional review board of Seoul National University (No. 2007/003-042). Informed consent was obtained from the participants.
1. Study Design
A quasi-experimental study with a non-equivalent control group, pre- and post-test design was conducted to evaluate the effects of a hybrid online and offline program to facilitate father-infant interactions based on assessments of infant development knowledge, father-infant interactions, and attachment of fathers to infants.
2. Study Participants
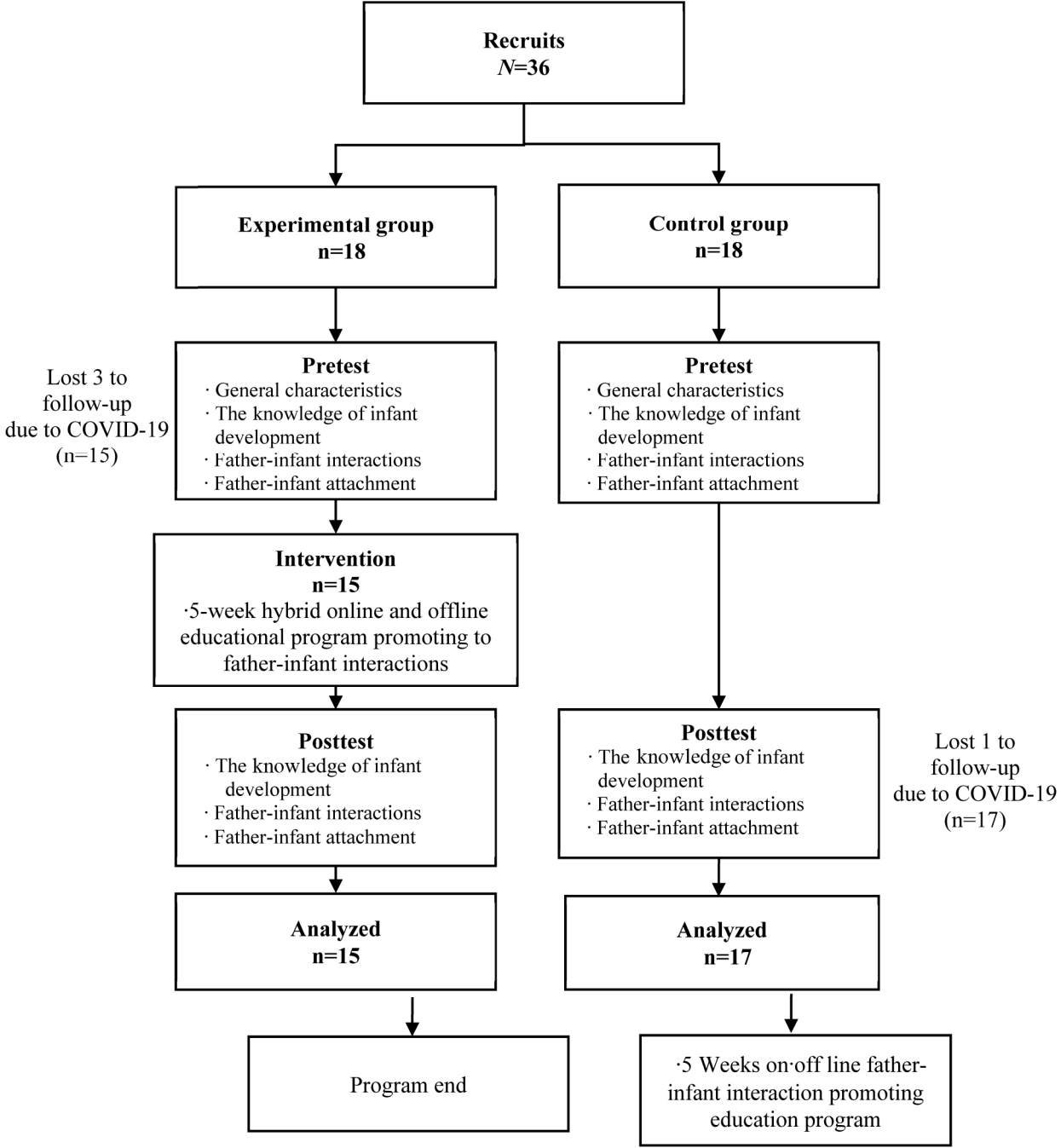
The fathers were spouses of participants in the Seoul Baby Health First Step Project. This community health project for the early stages of life was developed with financial support from the Seoul Metropolitan Government to reduce the health disparities in Seoul, and was implemented through Seoul autonomous districts public health centers. An analysis determined that in 2019, this project included about one-third of all children born in districts implementing the policy in Seoul. The sample size for this study was calculated using the G*Power program, with repeated-measures analysis of variance, a significance level of .05, a power of 80%, two measurements, and an effect size set to 0.30 with reference to a meta-analysis [12] and previous studies on paternal sensitivity and attachment [13]. The number of samples required for each group was 12. Considering a dropout rate of about 30%, 18 participants in the experimental group and 18 participants in the control group were required (Figure 1). The participants were collected among fathers whose children were between 8 and 24 weeks of age between January and June 2020 in families where the babies’ mothers participated in the Seoul Baby Health First Step Project. Fathers who had premature or low-birth-weight infants, or who could not communicate in Korean, were excluded.
At first, 36 fathers agreed to participate, among whom 18 were assigned to the experimental group and 18 to the control group according to project region. Three people in the experimental group withdrew during the intervention due to concerns about coronavirus disease 2019 (COVID-19), and one person dropped out before the post-test in control group. Thus, data from 15 participants in the experimental group and 17 participants in the control group, for a total of 32 participants, were used in the final analysis.
3. Measurements
1) General characteristics of study participants
The general characteristics were constructed by referring to the study of Kang and Park [14], considering the following characteristics of fathers and children that can affect child-rearing attitudes: father’s education level, yearly family income, infant age, infant sex, first childbirth, existence of secondary caregiver, previous participation of parent education experience.
2) Knowledge of Infant Development Inventory
The Knowledge of Infant Development Inventory (KIDI) was developed by MacPhee [15] to assess caregivers’ knowledge of infants and children from birth to 6 years of age and reconstructed by Kim [16] with 19 items in four sub-domains related to developmental norms from the 58 items in the original scale. This version includes five items in the sub-domain of cognitive development, five items on social-emotional development, five items on physical development, and four items on language development. The scoring is done as suggested by MacPhee [15], where 1 point is given for the correct answer and 0 points for incorrect answers and responses of “don't know”. Cronbach’s ⍺ was .67 at the time of tool development [15] and .77 in this study; hence, the reliability of the scale was acceptable.
3) Father-infant interactions
The father-infant interactions were observed using Barnard’s Nursing Child Assessment Satellite Program Training Scale (NCAST)[10]. This tool, which includes dimensions that affect the development of babies aged 0 to 36 months, can predict future development. The NCAST manual provides a list of activities for each developmental age, and it is included in the guidelines for children to engage in activities that are one step more challenging than the items that children can normally perform proficiently. In this study, among the developmental tasks that can be carried out within 100 days, such as playing with rattles, moving blocks from one hand to the other, and holding a duck doll with a quack sound, one activity suitable for the infant's individual development was selected and executed. The responses were divided into four sub-domains: sensitivity to cues (11 points), response to child’s distress (11 points), social-emotional growth fostering parenting behavior (11 points), and cognitive growth fostering parenting behavior (17 points). The infants’ responses are measured in terms of clarity of cues (10 points) and responsiveness to the caregiver (13 points)(yes and no dichotomies). These constitute the two caregiver and infant sub-domains, and a total of 73 items are scored. A “yes” response for each question is worth 1 point, while “contingency” is also worth 1 point; however, the total count of contingency questions-for which the caregiver’s action and the baby’s response happen at the same time-is 52. The range is 0-105 points. A higher score indicates a higher quality of father-infant interactions. The researchers received a research reliability score of .90 through the Barnard Center.
4) Father-infant attachment
The Maternal Attachment Inventory developed by Muller [17] to measure the mother's affectionate attachment to her infant was modified and supplemented by Han [18]. This instrument contains 26 items that the father’s attachment to the infant. Each item is scored on a 4-point scale ranging from 1 point for “almost never” to 4 points for “almost always,” yielding a total score that ranges from 26 to 104 points, with higher scores indicating higher parental attachment. At the time of development of this tool, Cronbach’s ⍺ was .85 [17], and in the study by Han [18], Cronbach’s ⍺ was .89, and in this study Cronbach’s ⍺ was .86.
4. Intervention
The intervention program was implemented in five sessions over a 5-week period. The first and fifth sessions involved two home visits (30 minutes each), where the fathers were individually educated by the researcher about how to interact with their infants. Written feedback on father-infant interactions was provided, and there were five online education sessions; the online components of the first and fifth sessions lasted 30 minutes each, while the other three online sessions each took 60 minutes (Table 1). The content of the online education focused on developing the caregiver’s sensitivity, building infant developmental knowledge, and recognizing the teaching loop during father-infant interactions. In other words, the program was conducted for a total of 5 weeks, and consisted of two home visits, written feedback with an individualized consultation on raising the baby, and online lectures for 5 weeks with content organized by the author. The basics of the lectures were adapted from Barnard [10], the founder of the University of Washington's Barnard Center and the NCAST developer, and adapted to the individual circumstances of the fathers of infants. The author has worked as a researcher for this project for 3 years and therefore has a high level of understanding of the project. She also holds an NCAST certification and specialized in pediatric nursing.
5. Ethical Considerations
Data were collected from July 26, 2020, to October 30, 2020, after receiving approval from the institutional review board of Seoul National University (No. 2007/003-042). Potential participants were enrolled when they agreed to participate in the study after receiving an explanation of the purpose and methodology of the study. However, since the study was related to a project in which the researcher was involved, this information was publicized to participants, and it was clarified that there would be no disadvantage due to not participating in this study. In addition, participants were notified in advance that the study could be stopped at any time, and an explanation was given of how data would be discarded and where to inquire about research-related questions or concerns. Image data were only accessed by the researcher using a fixed USB-to-PC connection. In addition, participants in the control group were given the opportunity to receive the intervention if they were interested in doing so after completing the post-test. The collected data will be used only to analyze the results of this study, anonymized data will be kept for 5 years, and scored videos will be disposed of after 1 year.
6. Data Collection
In the experimental group, an online preliminary survey was conducted immediately before the intervention, and a follow-up survey was conducted immediately after the last online education and home visit. Observations were performed after presenting the teaching situation in an unstructured form. Then, if the researcher made a direct home visit, the researcher recorded and observed a video directly using a mobile phone. A pre-observation was conducted after filling out a preliminary survey. The home visits took 30 minutes; filming required less than 10 minutes, research explanation and the completion of a written consent form took 10 to 15 minutes, and brief oral feedback and wrap-up were performed within about 5 minutes. Follow-up observations were conducted in the same format as the previous home visit, with the consent of the parents, if they had attended at least 60% of the video lectures. A real-time screen of the father-infant's activity video was transmitted online, without face-to-face interaction with the researcher. To prevent the effect of bias in the image scoring process, the scores used in the results were measured by a doctoral student at the Graduate School of Public Health (NCAST certificate holder) who did not know whether participants were in the experimental or control group. The intervention areas were relatively distant, so there was no risk of spread. In order to shorten the study period, data were collected from the experimental group and the control group at the same time. For the control group, feedback or online education on the results of image analysis (i.e., not videos) at two home visits (30 minutes) was provided after the investigation.
7. Data Analysis
SPSS for Windows version 23.0 (IBM Corp., Armonk, NY, USA), was used for the statistical analysis. Descriptive statistics were used to describe the demographic characteristics of the participants. The normality of the data distribution was tested using the Shapiro-Wilk test. The x2 test, the Fisher exact test, and the Mann-Whitney U test were used for between-group comparisons of data with a non-normal distribution. The variables were analyzed using generalized estimating equations (GEEs). The statistical significance level is normally p<.050 when scientific experiments are conducted under strict control, but a p-value of <.100 can be used in the field of the humanities and social sciences [19].
RESULTS
1. Homogeneity Testing of Demographic Characteristics
The paternal and infant characteristics showed no statistically significant differences between the experimental and control groups (p>.050). Father-infant interaction-related characteristics such as first baby, non-parental caregivers, and parental education also showed no statistically significant differences (Table 2).
2. Pre-homogeneity Testing for Outcome Variables
There were no statistically significant differences in the dependent variables, such as parent-child interactions, infantside parent interactions, infant developmental knowledge, and parent attachment score (p>.050), indicating that the two groups were homogeneous (Table 3).
3. Hypothesis Testing
• Hypothesis 1: infant development knowledge The GEE analysis conducted to investigate changes in the infant development knowledge score according to time between the experimental group and the control group showed no significant difference between the measurement time and the group interaction. Hence, hypothesis 1 was rejected (Table 4).
• Hypothesis 2: father-infant interactions The GEE analysis testing the difference in changes in the father-infant interaction score over time between the experimental group and the control group showed significant main effects for time (B=-5.40, p=.028, 95% confidence interval [CI]=-10.23 to -0.57) and group (B=-9.44, p<.001, 95% CI=-13.42 to -5.45), and the measurement time and group interaction showed a statistically significant difference at the significance level of .10 (p=.051) Hence, hypothesis 2 was supported (Table 4). The measurement time and group interaction for father-infant interactions from the infant aspect showed a statistically insignificant difference at the significance level of .10.
• Hypothesis 3: father-infant attachment The difference in the change of the attachment score over time between the experimental group and the control group was tested through a GEE analysis, as shown in Table 4. No significant difference in father-infant attachment according to the measurement time and group interaction was observed between the experimental and control groups. Hence, hypothesis 3 was rejected.
DISCUSSION
Fathers of infants are eager to learn how to improve the quality of their parenting and listen to nurses’ input on how to better interact with their babies [4]. However, at the same time, they may feel that they lack knowledge about the developmental characteristics of infants or find it difficult to deal with their babies [1]. In this study, although there was no difference in the amount of change in the infant development knowledge score between the experimental and control groups, the knowledge score related to infant development in the experimental group increased after the intervention. Having appropriate knowledge regarding children’s growth and developmental stages will influence fathers’ ability to provide appropriate care based on a sufficient understanding of their infants. There is a risk of child abuse when fathers repeatedly set unrealistic expectations and experience frustrations with their children due to insufficient knowledge about their children's development [20]. Conversely, if a father has sufficient knowledge about child development and a deep understanding of the child, this can be a key protection factor against child abuse or neglect [21,22].
In this study, it was confirmed that paternal education promoted father-infant interactions in the experimental group. Parent-child interactions were measured by the NCAST and were divided into caregiver and child sides. In this study, fathers’ education showed an effect on the caregiver side. It was expected that the father's sensitivity would increase through education targeting father-infant interactions, but it was expected that it would not be easy to show a change in the baby's clarity of cues or responsiveness to the caregiver in a short period of time. These results are supported by experimental data (Table 4). This intervention is significant in that it was provided at home and improved caregivers’ sensitivity and quality of care [23]. Although facility-based caregivers have opportunities to improve the quality of care through formal education, home-based caregivers are often excluded from education [24]. For fathers who are home-based caregivers for infants, where growth and development occur rapidly, improving their interactions with infants based on accurate knowledge about infant development will help them contribute to children’s health and development of children. An interaction-facilitating intervention could be provided to any mother or caregiver. Program-based education has been shown to increase caregivers’ sensitivity to infants and promote infants’ cognitive growth. Although there was no statistically significant change from the children’s standpoint, this program can be applied to a variety of subjects, including children with diseases [24]. In recent years, to improve the quality of interactions with children who have diseases, video-based feedback interventions have been used to provide an environment that promotes overall parent-child interactions, parental sensitivity, and children’s cognitive growth. These interventions have also been shown to be effective for responding appropriately to infants’ signals and behavior [25-27].
Video self-modeling refers to observing oneself to see one’s actions again, and this approach increases one’s concentration and emotional arousal. Parents are interested in education when they actively participate, and it was found that parents were very interested in receiving expert feedback on videos that they appear in [28,29]. Parents’ accurate interpretation and response to the baby's signals have a major influence on children’s behavioral development. Video-feedback interventions to promote positive parenting have also been utilized in other studies [30].
Participation in child-rearing research activities using online non-face-to-face video conferencing technology is also an attractive method for modern parents who are accustomed to using mobile applications for general communication [30,31]. It is reasonable to predict that non-face-to-face education will be more convenient and time-efficient for busy fathers. The significance of this study is that this educational program was provided in an appropriate format to meet the needs of these parents, knowing that internet is a major resource through which parents acquire and utilize information for raising children [29]. In the future, we hope that further research will identify ways of effectively delivering parental education by overcoming the limitations of time and distance and actively utilizing technology in the non-face-to-face era.
According to a recent study, parents’ emotional bond with their young children is assumed to be a motivational experience that defines the concept of a person. Attachment stability is a product of parent-child interactions rooted in the father's emotional bond to promote warm and responsive parenting behavior toward the infant [32]. Although the father's attachment to his infant is the key to sensitive and responsive care that promotes secure attachment in childhood, the short-term intervention provided in this study was not confirmed to have an effect on this variable. In addition, although developmental knowledge about infants according to age affects infant care and ultimately impacts attachment and interaction, it was difficult to identify external factors in this study due to factors such as poor control of external factors and a small number of subjects [33].
The fact that the fathers were recruited through their spouses could have resulted in selection bias. One of the major limitations of this study was the inability to control the spread of the mother's education in the course of the study, and the lack of impactful delivery due to the limitation of the technical quality of the videos. It will also be necessary for the researcher to play a role as a mediator or facilitator or to analyze improvements in the marital partnership through discussions of parenting issues with fathers.
Nevertheless, this study is meaningful in that it conducted an intervention to promote father-infant interaction targeting fathers, not mothers, and provided online and offline interventions to increase accessibility. The fathers also considered the NCAST to be an educational activity with a positive effect on the development of their babies and actively participated despite the coronavirus disease 2019 situation. It was also helpful that the researcher was able to establish rapport with parents by providing them with the opportunity to consult with the researcher on general health-related problems related to the baby during home visits.
CONCLUSION
This quasi-experimental study was conducted to determine the effects of applying an online and offline education program for fathers of infants to promote parent-child interactions. A significant difference was found between the experimental and control groups in the change in the father-infant interaction score after the program implementation. However, no statistically significant results were found according to group or time for infant developmental knowledge and parental attachment. These results imply that hybrid online and offline education can be encouraged to improve the quality of care provided by fathers at home. This will enable fathers to improve their interactions with children based on accurate knowledge of infant development through effective education. There is a need for supplementary follow-up research on programs to share experiences and increase participation in education.