Knowledge, confidence, and educational needs of newborn care among North Korean refugee women: a descriptive study
Article information

Abstract
Purpose
North Korean refugee women struggle with the double burden of adaptation and parenting as mothers in a new environment. This study aimed to identify the knowledge, confidence, and educational needs regarding newborn care among North Korean refugees, and to determine differences between these variables according to participants' characteristics.
Methods
Data were collected from September to October 2022, and 150 North Korean refugee women recruited using convenience sampling participated in the study. Descriptive statistics, the t-test, analysis of variance, and Pearson correlation analysis were used for data analysis.
Results
The mean scores were as follows: parenting knowledge, 14.97 out of 25; infection prevention knowledge and confidence, 20.09 out of 33 and 51.37 out of 80, respectively; and educational needs, 245.86 out of 310. Significant differences were observed in newborn care, knowledge, and confidence according to maternal age, educational level, family structure, and pregnancy history. Significant positive correlations were observed between the participants' newborn care knowledge, confidence, and educational needs.
Conclusion
Personalized educational programs should be implemented to enhance North Korean refugee women's confidence in newborn care, focusing on areas with low knowledge levels and high educational needs and enabling women to achieve healthy pregnancy and childbirth, and to parent well.
INTRODUCTION
In total, 33,834 North Korean refugees are reported to reside in South Korea, forming an important population group in today's South Korean society [1]. North Korean refugee women not only experience economic difficulties and unstable jobs, stress in the process of adjusting to life in South Korea, and traumatic experiences in the process of escaping from North Korea, but also lack social activities, social network formation, and a support system to obtain help and information [2]. In addition, North Korean refugee women experience many difficulties in raising children due to difficulties in acquiring information on pregnancy, childbirth, and childcare, as they do not have knowledge about the new society's childrearing methods and education system or have access to appropriate educational institutions [3]. Furthermore, the proportion of single-parent families among North Korean defectors is increasing, implying the possibility of poverty [4]. Although they have high expectations for their children, they experience difficulties in raising their children due to cultural differences and prejudice [4]. A previous study found that content related to pregnancy, childbirth, and childcare provided to North Korean refugee women at Hanawon, a settlement center for North Korean refugees, shortly after their arrival was neglected as a real problem in adapting to South Korean society [5]. Ultimately, a lack of information and understanding on pregnancy, childbirth, childcare, and postpartum care services for pregnant women can predict a lack of knowledge or skills on how to specifically perform the role of parents.
Knowledge of newborn care refers to maternal information on newborn care necessary for the growth and development of newborns [6]. A newborn is completely dependent upon its parents for survival and the mother, as the person who spends the most time with the newborn, faces considerable difficulties in fulfilling her role as a mother when she lacks knowledge about newborn care [7]. The maternal role for a newborn baby is not a competence that spontaneously emerges with the birth of a child, but a competence acquired through learning influenced by cultural and personal experiences [8]. Therefore, it is important that mothers are equipped with appropriate knowledge to achieve good parenting. Mothers who are well informed about newborn care are more confident in their parenting skills and have less parenting stress, which enables them to develop more effective parenting behavior [9].
In the process of parenting, health problems of the child not only negatively affect the child, but also increase the caregiver's burden [10]. It was reported that the research on prenatal care among marriage immigrant women focused on ways to maintain the health of newborns, such as newborn vaccinations and the management of health problems [11]. Furthermore, the vulnerabilities of North Korean refugee women include fear of contacting the healthcare system, cultural differences, housing insecurity, food insecurity, discrimination, health illiteracy and lack of readily available, and culturally appropriate educational materials. During pandemics, displaced persons suffer disproportionately from the threats posed by the infectious agent [12]. Since newborns cannot modify their environment or habits by themselves, parents play an essential role as caregivers in infection prevention by acquiring knowledge about diseases and newborns' health in order to protect them [13]. However, limited research has been conducted on parental knowledge and implementation regarding the performance of infection prevention, such as enhancing resistance to disease, managing and isolating infection vectors, maintaining and improving health conditions, and managing the environment. A systematic education program on infection prevention aimed at pregnant refugees from North Korea should be established. This should be preceded by a survey to identify the level of knowledge about newborn infection prevention among this population.
Newborn care educational needs encompass the acquisition of the knowledge and skills to care for newborns in a way that promotes their health, growth, and development [14]. The maternal role does not emerge spontaneously with the birth of a newborn, but is rather acquired through learning under the influence of cultural and personal experiences [15]. It is important to note that the benefits of education are commensurate with participants' interest in the educational content, so identifying these interests and selecting the educational content accordingly increases the efficiency of education [16]. Therefore, in order to foster maternal role attainment among North Korean refugee women, who are new members of our society, it is crucial to identify their level of knowledge about newborn care and assess their interests and educational needs in order to provide them with the appropriate education. Antenatal education of primiparas is of particular importance because primiparas experience greater difficulties than multiparas in relation to various newborn care skills such as feeding and burping, putting a baby to sleep, bathing, and appropriately interpreting a baby's crying [17].
According to a previous study, marriage migrant women need the most education in "safety accident prevention" and "toilet training", followed by "growth and development", "bathing", and "baby massage". It was found that education was also needed for "weaning food" [18]. Therefore, it is important for primiparas to learn about newborn care and develop their skills through firsthand experience. In addition to the basic education essential to take care of their newborns, primiparas should be provided with information that meets their educational needs. To enable systematic newborn care education, it is necessary to identify the level of parental knowledge of newborn care.
Studies conducted among mothers in multicultural families in Korea on pregnancy, childbirth, and parenting have examined women's level of knowledge about newborn care, pregnancy- and childbirth-related health care, and their educational needs in relation to rearing infants and young children [11,19]. These studies found that women of reproductive age in multicultural families had lower levels of knowledge about newborn care and parenting than Korean women [6,20]. However, little research has been dedicated to investigating the maternal knowledge of newborn care, educational needs, and related variables in North Korean refugee women. It is important to develop a systematic education program on pregnancy, childbirth, and parenting for North Korean refugee women who do not have easy access to pregnancy, childbirth, and parenting education, enabling them to develop good practices in newborn care. This study aims to provide basic data for developing a newborn care education program to enable North Korean refugee women to efficiently play their maternal roles.
This study aimed to prepare basic data for developing a newborn care education program by identifying the level of knowledge of newborn care (including infection prevention), confidence in newborn care and educational needs of North Korean refugee women. The objectives were as follows: 1) to identify the knowledge, confidence, and educational needs for newborn care of North Korean refugee women, 2) to analyze differences in knowledge of newborn care, confidence, and educational needs among North Korean refugee women depending on their general characteristics; 3) to compare the newborn care knowledge, confidence, and educational needs between women planning a pregnancy and primiparas, 4) to analyze the relationships between knowledge of newborn care, confidence, and educational needs in North Korean refugee women.
METHODS
Ethics statement: This study was approved by the Institutional Review Board (IRB) of Hannam University (No. 22-02-07-0622). Informed consent was obtained from all participants.
1. Study Design
This descriptive survey study examined the knowledge, confidence, and educational needs related to newborn care among North Korean refugee women who had infants or were pregnant or planning pregnancy, and determined differences according to participants' general characteristics. This study was reported in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [21].
2. Participants
North Korean refugee women registered with local community centers for North Korean refugees (Seoul, Gyeonggi Province, Daejeon) were the target population of this study. Participants who understood the study aims, methods, and questionnaires, and voluntarily agreed to participate in the study, were recruited by applying the following selection criteria: (1) women of reproductive age (18-50 years); (2) ability to communicate; (3) no chronic disability or disease; and (4) currently pregnant, planning a pregnancy, or parenting a healthy first baby less than 12 months of age. The sample size was estimated based on a previous study [22], taking into account invalid data due to errors and omissions by the nature of self-report questionnaires. A sample size of 120 was calculated with the G*Power 3.1 program using one-way analysis of variance (ANOVA), with the significance level set to .05, effect size .25, and power. 80. Considering a dropout rate of 20% the sample size was set to 144. Of the 165 North Korean refugee women who met the selection criteria, data obtained from 150 respondents were analyzed, after excluding 15 questionnaires with insincere responses to the survey.
3. Study Tools
1) Knowledge of newborn care
(1) Newborn care
Newborn care was measured using the tool developed by Lee and Oh [23] and modified by the researchers considering the level of understanding of the survey respondents. This is a self-report questionnaire consisting of 25 items that cover newborn feeding, belching, environment, jaundice, body temperature, abnormal symptom detection and care, umbilical care, and safety management. Each item is rated on a binary scale (1=correct answer, 0=incorrect answer), with the total score ranging between 0 and 25. Higher scores indicate a higher level of newborn parenting knowledge. Negatively-keyed items are reverse-scored.
The content validity of the tool was tested by a four-member expert panel (two professors of pediatric nursing, one head nurse in a neonatal intensive care unit, and one charge nurse), and the importance of each question was indicated on a 4-point scale. The content validity index (CVI) was calculated by assessing each of the items on a 4-point scale. Items that obtained less than 3 points were reformulated. The instrument's reliability was measured using the Kuder-Richardson 20 (KR-20). In this study, the KR-20 was .95.
(2) Infection prevention
Infection prevention was measured using the infection prevention knowledge scale developed by Lee and Kwon [24] and revised by Seo and Kim [25]. This 33-item self-report questionnaire consists of four subscales: handwashing, early detection, isolation and vector control, and immune defense. Each item is rated on a binary scale (1=correct answer, 0=incorrect answer/no response), with the total score ranging between 0 and 33 and higher scores indicating a higher level of knowledge of newborn infection prevention. The instrument's reliability was shown by Cronbach's ⍺ values of .94 in the study by Seo and Kim [25] and .91 in this study.
2) Educational needs for newborn care
Educational needs for newborn care were measured using the newborn care educational needs scale developed by Han [14]. This is a 62-item questionnaire rated on a 5-point Likerttype scale ranging from 1 (no interest at all) to 5 (very high interest). The total score ranges between 62 and 310, with higher scores indicating higher educational needs. The instrument's reliability was shown by Cronbach's ⍺ values of .98 in the study of Han [14] and .99 in this study.
3) Confidence in newborn care
Confidence in newborn care was measured using the newborn care confidence scale developed by An and Bang [26] and modified by the authors for the purpose of this study. This instrument is a 16-item questionnaire rated on a 5-point Likert-type scale ranging from 1 (no confidence at all) and 5 (very high confidence), with the total score ranging from 16 to 80 and a higher score indicating higher confidence. The instrument's reliability was shown by Cronbach's ⍺ values of .94 in the study by An and Bang [26] and .98 in this study.
4. Data Collection
Data were collected between September and October 2022 using self-report questionnaires distributed to the participants. Prior to data collection, permission was obtained from the heads of the South-North Hana Centers and Saejowi branches, a network providing medical counseling and resettlement support to North Korean refugees, after explaining the purpose of the study. Participants were recruited through online and offline posters. Participants' identities were not revealed to the heads of the individual centers, and the survey was conducted in the conference or counseling room of each center with the aid of working-level staff members. The purpose of the study and participants' anonymity and confidentiality were explained to the women, as well as the use of the survey results for academic purposes only and the participants' right to withdraw from the study at any time. The women were also informed that a summary of the study results would be made available. The principal investigator and a pre-trained assistant distributed the questionnaires to the participants to fill out directly, and then immediately retrieved them. If participants needed help in the process of filling out the questionnaire, the research director or assistant helped them complete it. The questionnaires were collected immediately after completion. If any of the participants reported discomfort while completing the questionnaire, particularly the pregnant participants, they were allowed to rest in a comfortable armchair, and the principal investigator assessed the participants' condition, including vital signs, and decided whether they could continue. In each case, the participant concerned received an explanation that she could withdraw from the survey without incurring any disadvantages. It took 15 to 20 minutes to complete the questionnaire. Following completion, each participant was given a small token of appreciation (mobile coffee coupons or baby products).
5. Data Analysis
The data were analyzed using the SPSS 21.0 program (IBM Corp., Armonk, NY, USA). The results of the analysis of differences in the dependent variables (knowledge of newborn care, confidence, and educational needs for newborn care) according to the general characteristics of the women were presented as frequency, percentage, mean, and standard deviation. ANOVA and the Kruskal-Wallis test were used to evaluate the relationships between the dependent variables. The Bonferroni correction was used for post-hoc analysis. Pearson correlation coefficients were used to analyze intervariable correlations.
RESULTS
1. Participants' General Characteristics and Differences in the Variables According to the General Characteristics
Participants' general characteristics were as follows: most participants were in their 30s (n=88, 58.7%), and 92 (61.3%) had graduated from middle or high school (completed formal education in South Korea). Family structure was categorized as currently living alone (single or married) (n=93, 62.0%), the predominant duration of residency in South Korea was 5 to 10 years (n=78, 52.0%), and the majority of participants were planning pregnancy at the time of study participation (n=122, 81.3%).
Significant differences in knowledge of newborn care were observed according to age, educational level, family structure, and pregnancy history. The scores for knowledge of newborn care were significantly higher (x2=30.69, p<.001) in the participants in their 30s and 40s than in those who were younger than 30 years (0.67±0.27, 0.78±0.25, and 0.37±0.33, respectively). Significantly higher scores for knowledge of newborn care (x2=24.15, p<.001) were observed among participants with a college/university or graduate school degree (0.83± 0.23). Participants who lived alone had significantly lower scores than those who lived with a spouse group and those in civil partnerships (0.49±0.32 vs. 0.75±0.24 vs. 0.88±0.09; x2=36.93, p<.001). Mothers with one infant scored significantly higher than those planning a pregnancy (0.85±0.15 vs. 0.54± 0.32; x2=22.32, p<.001). Infection prevention knowledge scores were significantly higher in participants in their 30s (0.65±0.20; x2=9.96, p=.007); with a college/university or graduate school degree (0.73±0.11; x2=6.49, p=.039), who were living with a spouse (0.70±0.18; x2=14.98, p=.001), and who had one infant (0.76±0.12; x2=16.76, p<.001) than in their respective counterparts.
Significant differences were also observed in confidence in newborn care according to age, educational level, family type, and pregnancy history. Significantly higher scores for confidence in newborn care were observed in participants in their 30s and 40s than in those who were younger than 30 years (3.40±0.79 and 3.71±0.61, respectively, vs. 2.60±1.25; x2=16.93, p<.001). Significantly lower scores were obtained for confidence in newborn care in those with an elementary education or lower (2.49±1.13; x2=27.88 p<.001), those who lived alone (2.88±1.03; x2=28.35, p<.001), and those who were planning a pregnancy (3.10±1.03; x2=12.32, p=.002).
Significant differences were observed in educational needs for newborn care according to participants' educational level, with lower scores obtained in participants with an elementary education or lower than in those with a middle-high school education (3.45±1.19 vs. 4.13±0.52; x2=8.90, p=.012) (Table 1).

General Characteristics of Participants, Their Degree of Knowledge and Confidence in Newborn Care, and Educational Needs for Newborn Care (N=150)
2. Knowledge of Newborn Care, Confidence, and Educational Needs for Newborn Care
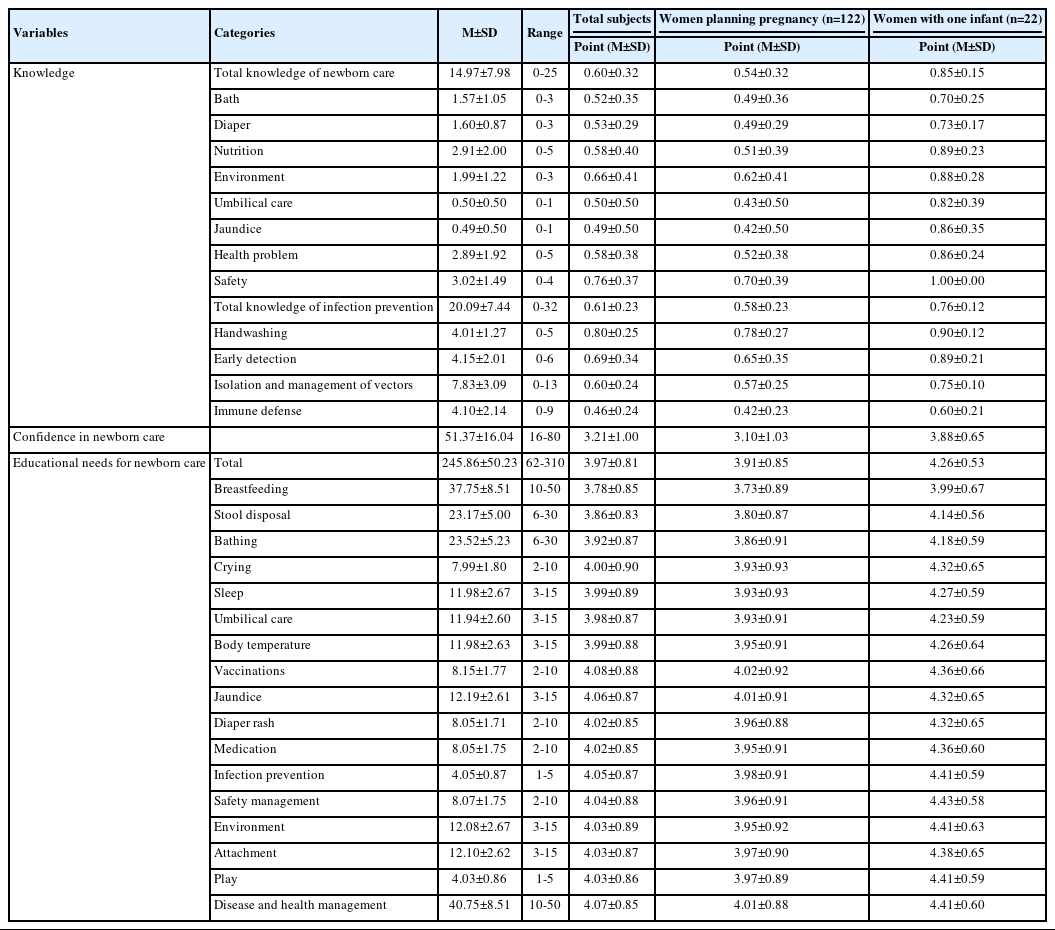
The overall mean score for the parenting knowledge domain of newborn care knowledge was 14.97±7.98 out of 25 points (0.60±0.32/1). Among the subscales, safety management had the highest score 0.76±0.37/1 and jaundice care had the lowest score (0.49±0.50/1), followed by umbilical cord care (0.50±0.50/1) and bathing (0.52±0.35/1). The overall mean score for the infection prevention knowledge domain of newborn care knowledge was 20.09±7.44 out of 33 points (0.61±0.23/1). Among the subscales, handwashing had the highest score with 4.01±1.27 (0.80±0.25/1) and immune defense had the lowest score with 4.10±2.14 (0.46±0.24/1). The overall mean score for confidence in newborn care was 51.37±16.04 out of 80 points (3.21±1.00/5). The overall mean score for newborn care educational needs was 245.86±50.23/310 points (3.97±0.81/5). Among the subscales, vaccinations had the highest score of 8.15±1.77 (4.08±0.88/5), followed by disease and health management (40.75±8.51 or 4.07±0.85/5), and breastfeeding (37.75±8.51 or 3.78±0.85/5) and stool disposal (23.17±5.00 or 3.86±0.83/5), which had below-average scores (Table 2).
Knowledge of Newborn Care, Confidence in Newborn Care, and Educational Needs for Newborn Care (N=150)
3. Comparison of Knowledge of Newborn Care and Educational Needs for Newborn Care between Women Planning a Pregnancy and Primiparas
Newborn care knowledge and educational needs were compared between women planning a pregnancy and primiparas, and significant differences were found in the newborn care knowledge and confidence scores. Women planning pregnancy obtained above-average scores in the knowledge subcategories of safety management (0.70±0.39) and environment (0.62±0.41) and below-average scores in jaundice care (0.42±0.50) and umbilical cord care (0.43±0.50). Primiparas (with an infant ≤12 months) obtained full scores in safety management (1.00±0.00), followed by nutrition (0.89±0.23), stool disposal related to diaper changes (0.73±0.17), and bathing (0.70±0.25). Among the infection prevention subscales, both the pregnancy planning and primipara groups obtained the highest scores in handwashing (0.78±0.27 and 0.90±0.12, respectively), and the lowest scores in immune defense (0.42± 0.23 and 0.60±0.21, respectively).
Regarding newborn care educational needs, women planning pregnancy showed the highest educational needs for vaccinations (4.02±0.92), followed by jaundice care (4.01±0.91) and disease and health management (4.01±0.88), and the lowest educational needs for breastfeeding (3.73±0.89), followed by stool disposal (3.80±0.87) and bathing (3.86±0.91), scoring below average. Primiparas showed the highest educational needs for safety management (4.43±0.58), followed by environment management (4.41±0.63), disease and health management (4.41±0.60), and infection prevention (4.41±0.59) and playing (4.41±0.59), and the lowest educational needs for breastfeeding (3.99±0.67), as in the women planning pregnancy, following by stool disposal (4.14±0.56), bathing (4.18± 0.59), and umbilical cord care (4.23±0.59), with below-average scores (Table 2).
4. Correlations between Knowledge, Confidence, and Educational Needs for Newborn Care
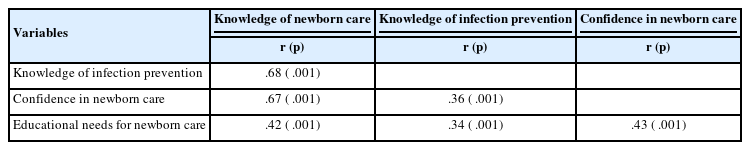
Correlation analysis revealed the following intervariable correlations: (1) among the knowledge domains, knowledge of newborn care had moderate positive correlations with infection prevention knowledge (r=.68, p<.001), confidence in newborn care (r=.67, p<.001), and educational needs (r=.42, p<.001); (2) infection prevention knowledge showed mild positive correlations with confidence in newborn care (r=.36, p<.001) and educational needs (r=.34, p<.001); and (3) confidence in newborn care displayed a moderative positive correlation with educational needs (r=.43, p<.001). These correlations indicate the following: (1) higher levels of knowledge of newborn care were associated with higher levels of infection prevention knowledge and educational needs for newborn care; (2) higher levels of infection prevention knowledge were associated with greater confidence in newborn care and educational needs for newborn care; and (3) greater confidence in newborn care was associated with educational needs for newborn care (Table 3).
Correlations among Knowledge of Newborn Care, Confidence in Newborn Care, and Educational Needs for Newborn Care (N=150)
DISCUSSION
This study was conducted to provide basic data for developing a newborn care education program to help North Korean refugee women better carry out their maternal roles. To this end, levels of knowledge of newborn care and infection prevention knowledge were examined among North Korean refugee women who had infants under 12 months of age, were pregnant, or were planning a pregnancy, as well as their confidence in newborn care and educational needs. A comparative analysis of future mothers planning a pregnancy and women with one infant under 12 months of age was conducted to identify directions for future newborn care education and to develop education tailored to the needs of the trainees. Among the subscales of knowledge of newborn care, safety management had the highest score (0.76/1). Lee and Oh [23] measured newborn care knowledge, albeit using a different tool, among mothers in multicultural families and obtained a similar score (0.63/1). The knowledge scores for individual subscales were also similar to those previously reported [23,27], with below-average scores in jaundice care, umbilical code care, bathing, stool disposal, feeding, and health problems, which were thus identified as items requiring education to ensure the healthy growth and development of newborns.
Significant differences in the knowledge of newborn care were observed, with participants younger than 30 years, those with an elementary education or lower, and those who lived alone scoring significantly lower than their counterparts. These results are consistent with those reported by Kim et al. [22] and Lee and Oh [23], in which the youngest group (<25 years) of mothers in multicultural families scored lowest in newborn care knowledge, and those reported by Jeon et al. [20], who stated that women with children had a higher level of knowledge of child-rearing. These findings may be explained by experiences of childbirth, antenatal education, and child-rearing.
In the present study, women planning pregnancy and women with one infant were compared. In the knowledge of newborn care, women planning pregnancy achieved high scores for safety management and environment management and low scores for jaundice care and umbilical cord care. Similarly, women with one infant achieved high scores in safety management (1.0 out of 1.0), followed by feeding, and low scores in stool disposal (diaper changes) and bathing. Although women with one infant achieved higher scores in jaundice care and umbilical cord care owing to their experiences, low scores were observed in stool disposal and bathing despite the fact that these are part of the daily routines of mothers parenting infants.
In this study, primiparous mothers with infants showed different patterns of scores from women planning pregnancy because they had experienced jaundice and umbilical cord management. However, even among those raising newborns or infants, their low knowledge in the area of diapers and bathing indicates that they were unable to cope with routine daily tasks such as changing diapers and bathing. There is a possibility of incorrect care in the family, so support is needed to help mothers acquire correct parenting knowledge. These findings suggest the need to support North Korean refugee women, both mothers and future mothers, to acquire correct parenting knowledge.
Given the specific characteristics of North Korean refugee families, which are characterized by a high proportion of single-parent families and exposure to a different culture and customs, parenting difficulties are associated with the lack of personal and system support. A lack of knowledge of newborn care lowers confidence in newborn care, leading to inappropriate parenting behavior, which in turn impairs parental efficacy. Therefore, educational intervention is required from the pregnancy planning stage, and vulnerable groups (those younger than 30 and low-education groups) should be provided with personalized education tailored to their particular needs.
The mean score for infection prevention knowledge was 20.09 out of 33 points. This was significantly higher than the score of 16.68 reported by Seo and Kim [25] using the same tool in their study on married immigrant Vietnamese women, and this difference may be explained by variation in participants' understanding of the questionnaire between participants using their native language and foreign language users. In addition, since the survey was conducted after the spread of coronavirus disease 19 (COVID-19), it may also reflect the circumstantial trait of increased information acquisition related to infection prevention and active coping with infection risk. Among the subscales, handwashing had the highest score and the immune defense domain had the lowest score.
Regarding the differences according to participants' general characteristics, those younger than 30 years, with an elementary education or lower, and living alone scored significantly lower than other groups. These results support the findings of Lee and Kwon [24]. In terms of pregnancy history, women planning pregnancy scored significantly lower than the women with one infant. At the subscale level, both groups scored highest in handwashing and lowest in immune defense. This most likely reflects the high awareness of and adherence to COVID-19 infection prevention routines and highlights the importance of expert involvement in domains such as the human immune system and defense mechanisms. Children learn through imitation, and maternal health behavior becomes a model for them to gain beneficial health habits [24]. Therefore, it is important for mothers to strengthen immunity at home, maintain and improve their health status, manage the environment, and block propagation routes of disease vectors in daily life through correct infection prevention knowledge.
North Korean refugees face limitations in the acquisition of medical information and access to support systems, and find it difficult to use healthcare facilities [28]. Moreover, when refugee women become ill, they prefer using medication based on self-diagnosis and folk remedies to consulting doctors [28]. It is therefore all the more important to enhance correct infection prevention knowledge of North Korean refugee women lest their children should learn such incorrect health behaviors. In particular, it is necessary to develop personalized education to increase the effectiveness of education for young women (<30 years of age) and those with low educational levels, and to support them so that they can boost their immune responses and defense ability and practice infection prevention in their daily life.
The score for confidence in newborn care, measured as a proxy of newborn care confidence, was 3.21/5, which is similar to the score of 3.3/5 among primiparas and multiparas reported by Chung and Joung [29] and the score of 64/100 for confidence in the maternal role obtained from early postpartum mothers in the study by Ha and Kim [30]. Younger age, lower educational level, and a single household were associated with lower confidence in newborn care. These results partially support the findings by Chung and Joung [29] that older maternal age was associated with higher maternal confidence among multiparas and that a higher educational level and level of social support were associated with higher maternal confidence among primiparas.
Under the dual burden of adapting to South Korean society and fulfilling their maternal roles, single women or married women living alone are considered to have a high emotional burden of newborn care without the support of a spouse or other family members. Since greater parenting confidence leads to greater parenting success, newborn care education services for North Korean refugees should include content that boosts parenting confidence.
Among the subscales of educational needs for newborn care, vaccinations had the highest score, followed by disease and health management, and breastfeeding and stool disposal had below-average scores. The overall score was slightly lower than the score reported by Lee and Oh [23] among mothers in multicultural families, who showed high scores for sleep and health management and low scores for nutrition. It is necessary to develop a newborn care education program tailored to participants' sociocultural and educational characteristics and needs. In this study, educational needs for newborn care significantly varied according to the educational level: women with an elementary education or lower had significantly lower scores than those with middle-high school education. Considering that higher educational needs are associated with a greater amount of knowledge to be acquired [22], North Korean refugee women with a low educational level need to be encouraged to actively participate in education programs so that they can benefit sufficiently from newborn care education services.
The finding of significant differences between women planning pregnancy and women with one infant is also consistent with previous studies [20,23] that have revealed differences in educational needs between women with and without children. Parenting mothers have increased needs for information to overcome difficulties encountered in the course of childrearing, which may have resulted in higher scores for educational needs. Women planning pregnancy had the highest educational needs for vaccinations, followed by jaundice care and disease and health management, and the lowest educa tional needs for breastfeeding, followed by routine care such as stool disposal and bathing (below-average scores). Although the women with one infant had high educational needs for safety, environment, disease and health management, infection prevention, and play, they had the lowest educational needs for breastfeeding and below-average educational needs for stool disposal and bathing, as was the case with women planning pregnancy.
These differences in educational needs between the two groups suggest that educational needs vary depending on the experience of newborn care. Moreover, the contradiction between low educational needs and the lowest newborn care knowledge in stool disposal (diaper changes) and bathing is consistent with the assumption that North Korean refugee mothers are likely to play the maternal role of newborn care with limited knowledge and incorrect confidence. However, both groups had the lowest educational needs for breastfeeding. Although a binary (yes-no) question is insufficient to identify maternal awareness of the importance of breastfeeding, breastfeeding education should be provided after identifying maternal knowledge and confidence regarding breastfeeding. As the educational effect is commensurate with the participant's interest in the content, it is important to investigate the interests of participants, evaluate their needs, and provide personalized education based on these findings. In this context, it is essential to provide North Korean refugee women, who face difficulties with pregnancy, childbirth, and parenting due to insufficient adaptation to the new society and culture and lack of personal support [3], with the necessary educational support conducive to the healthy development of their children and high-quality parenting.
Intervariable correlation analysis revealed that a higher level of knowledge of newborn care was associated with higher infection prevention knowledge and confidence in newborn care and greater educational needs. Furthermore, a higher level of knowledge of infection prevention was associated with higher confidence in newborn care, which in turn was linked to greater educational needs. This finding is consistent with the results of Kim et al. [22], who demonstrated a positive correlation between knowledge and confidence related to newborn parenting. However, this finding contradicts the results of a study on mothers in multicultural families, according to which knowledge of newborn care had no significant correlation with educational needs for newborn care [23]. Since North Korean defectors and women from multicultural families do not have the same socioeconomic characteristics, the possibility that the high knowledge score was not due to chance or that other external factors mediated or interacted cannot be ruled out.
In addition, since there is a difference between knowledge and needs, it should be recognized that educational content cannot be composed only based on the relationship between knowledge scores and requirements. It is necessary to organize education after confirming what the subjects know and what they are particularly interested in learning. There is a lack of previous research on this relationship, underscoring the need for additional research on mothers from multicultural families, including North Korean defectors.
North Korean refugee women who go through pregnancy, childbirth, and parenting are under the dual burden of adapting to an unfamiliar environment and playing the maternal role amidst complex and unpredictable experiences and unstable conditions, including the trauma incurred during the defection process. Although they can gain information on child-rearing through various information channels, the information they obtain may be flawed. A previous study [28] demonstrated that North Korean defectors had very low health literacy and found it difficult to discern accurate and relevant information, even when equipped with a certain level of health literacy and educational level. Importantly, their political and sociocultural background profoundly impacted their parenting behavior [31]. In order for proper parenting to take place, correct knowledge is required, and newborn care education is essential for the healthy growth and development of North Korean refugee women themselves and their children. Such education will also be vitally important for those who experience substantial confusion and conflict in adapting to South Korean society, in order to be able to enjoy the quality of life provided by Korean society.
Limited research has been conducted on newborn care knowledge, confidence, and educational needs and care-related infection prevention among North Korean refugees. This study is the first attempt to identify the knowledge of newborn care and confidence among North Korean refugee women of reproductive age and to examine knowledge of newborn care, confidence, and educational needs in women planning pregnancy and primiparas (with infants less than 12 months of age). However, because the population of North Korean refugee mothers is limited to some regions, the findings of this study cannot be generalizable to all North Korean refugee mothers. Therefore, future studies will have to be conducted with larger sample sizes.
Based on these limitations, the following proposals for further research are made: First, to date, studies on the child-rearing of North Korean refugees have focused on mothers, and future research may also include North Korea refugee fathers, which would allow mother-father comparisons. Second, in the evaluation of newborn care knowledge, confidence, and educational needs, it was not possible to identify previous educational status. Therefore, it would be necessary to check whether the participating women had previously received education on pregnancy, childbirth, and parenting. Third, following the finding of Kim et al. [22] that willingness to participate in education varied according to participants' occupation, it is important to examine job-dependent knowledge, confidence, and educational needs. Fourth, it is proposed to develop a newborn care program for North Korean refugee mothers reflecting their social and cultural characteristics and educational needs and to test the effectiveness of the program. A community-based newborn care education intervention will be a nursing intervention that could help North Korean refugee women better cope with various difficulties in newborn care and increase their confidence in newborn care.
CONCLUSION
This study aimed to identify the knowledge of newborn care, confidence, and educational needs for newborn care among North Korean refugee women, who have limited opportunities to acquire parenting-related information and limited support, and to provide basic data for developing a newborn care education program tailored to their characteristics. Since insufficient parenting knowledge can lower confidence in parenting and obstructs parenting behavior, which can lead to parenting stress [32], there is a compelling need to provide North Korean refugee women with personalized education programs tailored to their educational needs and centering on low knowledge and high education need areas in order to help them acclimate to the new society of South Korea, support them through pregnancy, childbirth, and parenting, and promote confidence in newborn care.
A proactive advertising and supportive campaign is necessary to induce North Korean refugee women of reproductive age to actively participate in newborn care education programs after their settlement within the local community in order to promote routine newborn care skills such as bathing, ideal feeding, and umbilical cord care, and to increase their interest in breastfeeding. Lastly, community-based newborn care education interventions where the developed program is linked to agencies affiliated with the government and local governments, North Korean refugee adaptation centers in local communities, and private organizations could help North Korean refugee women with various difficulties that arise when caring for newborns. These results provide basic data for newborn care education that can help not only North Korean refugee mothers, but also their families.
Notes
Authors' contribution
All the work was done by In-Sook Lee.
Conflict of interest
No existing or potential conflict of interest relevant to this article was reported.
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (No. NRF-2022R1H1A2005288).
Data availability
Please contact the corresponding author for data availability.
Acknowledgements
None.