INTRODUCTION
Children grow and develop rapidly and continuously in the first years of life [1]. While a child's body continues to grow and develop throughout the preschool years, the child's central nervous system gradually develops at an unparalleled rate. As a consequence, the child's development is accelerated to attain age-appropriate developmental milestones [2]. The child's entire ecosystem, from close elements (e.g., the family) to distant components (e.g., the global environment), plays a significant role in determining the child's early development [3].
Experiencing undesirable environmental conditions can result in developmental disabilities (DDs) in children. Children who do not meet developmental milestones compared to other children their age are deemed to have DDs [4]. A delay might occur in only one domain, such as gross motor, fine motor, language, social-emotional, or problem-solving skills, or it can occur in multiple domains. Significant delays in two or more domains of development that afflict children under the age of 5 years are referred to as global developmental delay (GDD) [5]. The community is impacted by the consequences of DDs on different levels, including personal, social, economic, and ecological [6,7]. Therefore, it is essential to investigate the risk factors of DDs from various viewpoints, including those of the child, parents, family, caregivers, and significant others.
Globally, the number of children who have ever been diagnosed with DDs or developmental delays has increased significantly [8]. According to the Lancet Global Health 2016 study, poverty and stunting prevent 43% of children under the age of 5 years from reaching their developmental potential in low- and middle-income countries (LMICs) [9]. According to data from developed countries, DDs affect 10% to 15% of children under the age of 5 years [10], while GDD affects 1% to 3% of children under the age of 5 years [4]. During 2014 to 2016 in the United States of America, the prevalence of DDs significantly increased from 5.76% to 6.99% [8]. Moreover, according to studies conducted in the United Arab Emirates (UAE) and Saudi Arabia, the prevalence of DDs was significant as well, at 8.4% and 16.4%, respectively [11,12].
Early child development is a critical determinant of one's potential throughout one's life, particularly in terms of health, education, and economic standing [13]. The focus of worldwide efforts has recently switched to the 2030 Sustainable Development Goals, which emphasize the need for "nurturing care" in boosting early child development [9]. Because of the importance of early detection and prevention of DDs, many developed countries have made it a policy to track children's developmental milestones from birth through school age. However, as evidenced by a thorough literature analysis, this problem remains widespread among developing countries, particularly in the Arab world [8,14].
According to the Regional Office for the Eastern Mediterranean of the World Health Organization, in 2021 there were around 679 million people living in the Arab world, which includes 22 countries and territories, including Algeria, Bahrain, Comoros, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, the UAE, Yemen, and Palestine (the Gaza Strip and West Bank). Although the countries in the Arab world vary considerably in terms of their economic situations, they are all united by a shared language, culture, and religion [15]. In order to investigate the prevalence of DDs among preschoolers in the Arab world, this study conducted a narrative review of the relevant literature.
There are few published studies that address the prevalence and risk factors of DDs in preschool-aged children in the Arab world, and there are less data on their prevalence. In light of this, the goal of this investigation was to assess the prevalence and risk factors of DDs among preschool children in the Arab world. Through this narrative review of DDs among preschool children in the Arab world, the researchers aimed to develop a regional protocol and early screening and intervention programs for all preschool children for any DD and to create a follow-up care program to optimize preschool children health and limit the burden of DD-related problems in adulthood.
METHODS
Ethics statement: This study was a literature review of previously published studies and was therefore exempt from Institutional Review Board approval.
1. Study Design
This narrative literature review was designed to review the estimated prevalence, risk factors, and assessment methods for DDs among preschool children in the Arab world. This study followed the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist [16].
2. Research Method and Literature Search
Between January 2001 and December 2021, a search was carried out in six major worldwide databases, including PubMed, Scopus, Cochrane Library, CINAHL, Science Direct, and Google Scholar, for all published articles on DDs among preschool children in the Arab world. On December 25, 2021, the first search was started, and on January 25, 2022, the last search was completed. Medical Subject Headings (MeSH) terms were used to identify research articles; the search keywords included "development disabilities" and "child, preschool". To find related publications, the Boolean operator "AND" was used to search these terms together. The reference lists of eligible studies were also searched. The population, exposure, and outcomes (PEOP) search approach was employed in this study. "Preschoolers", "developmental disabilities", "prevalence", and "risk factors", combined with the "Arab world" OR (Middle East, Arabian Gulf, and specific country names) were all included in the keyword search. The search items were combined using the Boolean operators "OR" and "AND". After reviewing 25 publications that explored the prevalence of DDs and risk factors for their occurrence in preschool children, 14 articles that met the specified inclusion criteria were selected.
3. Inclusion and Exclusion Criteria
This review included any study design reporting the prevalence of DDs or GDD among preschool children in the Arab world, written in English, and with full-text papers published within the last 20 years. This review did not include abstracts, conference papers, editorials, case reports, or articles for which the full text could not be obtained (even after emailing the corresponding author).
4. Study Outcome
The outcome of this review was the estimated prevalence of DDs, which was determined by the percentage of preschool children who performed below the age-appropriate cut-off point for each developmental domain evaluated in the study. The prevalence of individual developmental domains and global delay was estimated [17]. According to the United Nations, preschool children are individuals who are 3 to 5 years old [14]. The 22 countries and territories that make up the Arab League were considered the Arab world, as were countries and people who speak Arabic throughout North Africa and Western Asia.
5. Data Extraction and Data Synthesis
To avoid bias in the literature review and research, two reviewers independently searched and evaluated the literature. Disagreements were then resolved through discussions. To ensure consistency, two reviewers retrieved data from eligible studies. When accessible in the reports, the development assessment tool was also extracted, along with risk factors that were reported to be significantly associated with DDs (Table 1). Additionally, data on DD prevalence were retrieved and provided in accordance with the original studies (Table 2).
RESULTS
1. Overview of the Selected Research
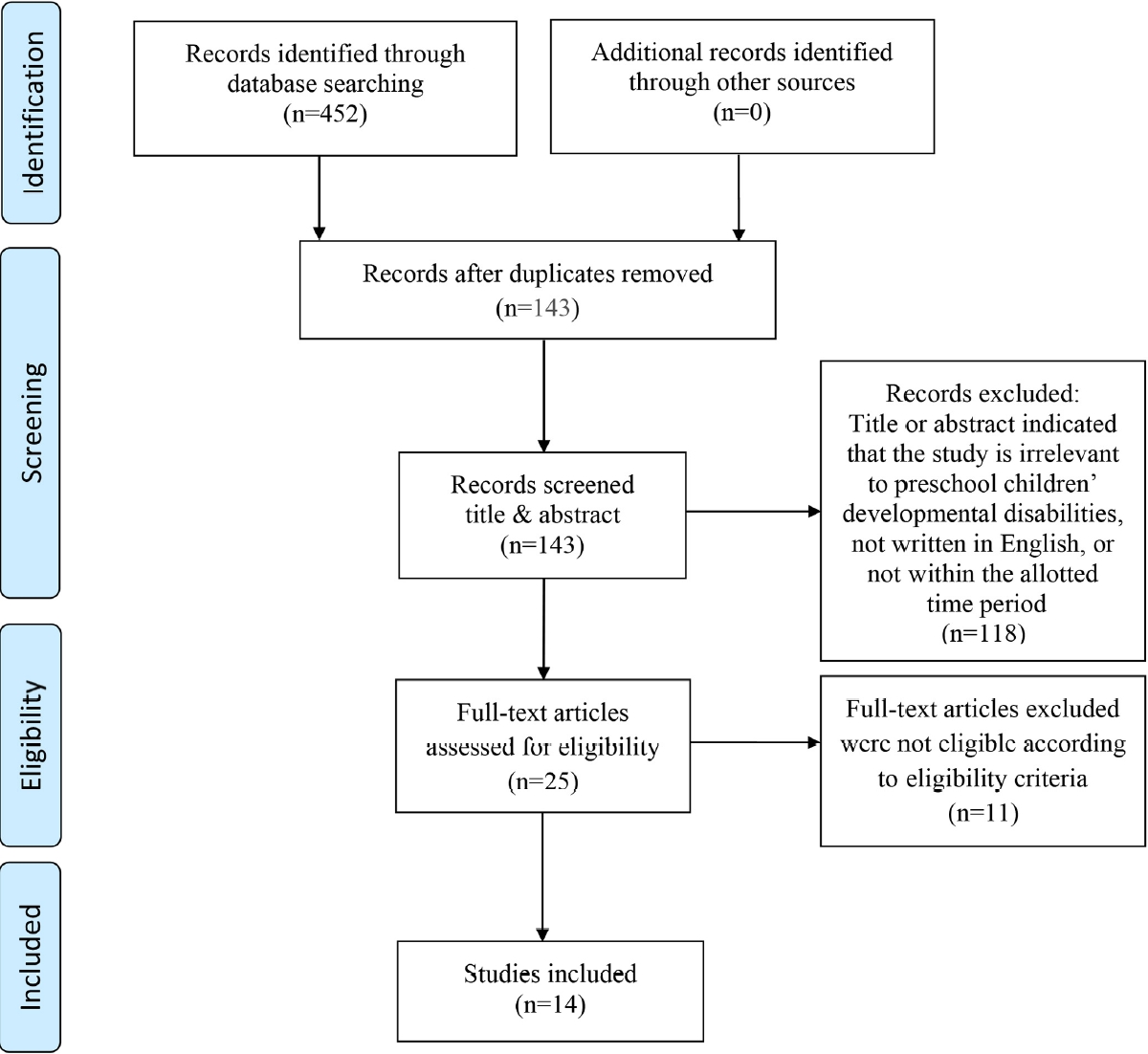
The literature search procedure was laid out in a PRISMA flowchart [18]. Upon combining the study variables, a total of 452 published publications were located, retrieved, and evaluated. From those, 118 articles were discarded after 143 duplicate records were eliminated through title and abstract screening because they were irrelevant, were not written in English, or had not been published within the required dates. Next, the eligibility of 25 full-text papers was evaluated in accordance with the inclusion and exclusion criteria. Eleven full-text articles were disqualified because they did not meet the requirements for inclusion. The final analysis included 14 studies (Figure 1). A descriptive analysis of the selected studies was conducted. The country name, DD prevalence, assessment tools, and the reported risk factors were recorded. Fourteen studies from 12 countries in the Arab countries met the inclusion criteria and were summarized (Table 1). One study was available from Jordan [19], the UAE [11], and Oman [20]; two each were from Lebanon [21,22], Iraq [23,24], Egypt [25,26], and multiple LMICs [27,28], while three were from Saudi Arabia [12,29,30]. Most of the included studies were quantitative and used a cross-sectional research design (n=11) [11,12,21,23-28], while two used prospective designs [20,30], and two others used a retrospective design (Table 1) [19,29].
The main objectives of the 14 included studies were to identify the prevalence and risk factors of DD among preschool children, and the studies used self-reported questionnaires in addition to developmental screening measurements. In this review, Four studies used the Denver Developmental Screening Test [11,21,24,30] and five studies used the Age and Stage Questionnaire [12,22,23,25,26]. Two studies used the Early Child Development Index [27,28], and one study used the Griffith Mental Development Scale [29]. Two studies did not use any instruments, as the objective of these studies was to determine common etiologies among DD patients [19,20]. In the included literature, DDs were defined adequately according to the American Academy of Neurology and the practice committee of the Child Neurology Society guidelines [5].
2. Estimated Prevalence of Developmental Disabilities among Preschool Children
The overall crude prevalence of DD reported in nine studies was 27.5% (n=11,791/42,890). Five of the reviewed studies were excluded from the crude prevalence calculation because the prevalence of DDs was not reported [19,20,22,24,29]. Significant regional and national differences were found in the prevalence of DDs. The prevalence of DDs among preschool children varied significantly among countries, from 3.4% in Egypt to 39.2% in Saudi Arabia [24,30]. Within populations, the prevalence was 16.4% to 39.2% in Saudi Arabia [27,30]. Similarly, the prevalence ranged from 26.5% to 31.6% in Palestine [27,28]. Overall, the most prevalent domains of DDs were the personal/social-emotional and intellectual/cognitive domains (Table 2).
3. Risk Factors of Developmental Disabilities among Preschool Children in the Arab World
1) Child-related factors
Child-related risk factors for DD were sex, prematurity, and child exposure to physical discipline and deprivation.
All studies included male and female participants, and a substantial relationship was identified between the prevalence of DD and sex. Five studies reported that boys were more likely than girls to have DD [22-26], and one study indicated that the mean development scores were higher in girls than in boys [22].
Prematurity [21,24,30], birth weight less than 2.5 kg [24,29], and artificial feeding before 6 months of age [12] were identified as risk factors for DDs. Finally, exposure to physical discipline and deprivation, which were investigated in a survey conducted in multiple LMICs, showed cross-nationally distinct associations with the risk of socio-emotional and cognitive delays [27].
2) Maternal-related factors
History of pregnancy, birth, and perinatal complications were identified as substantial risk factors for DDs in preschool children, according to five of the studies analyzed; Asphyxia, jaundice, and congenital disorders were significantly associated with DDs in preschool children [11,19,23,24,29]. In addition, a lower level of maternal education was identified as a risk factor by five studies [11,12,22,24,26]. Lastly, the maternal working status (non-working mother) was associated with lower mean development scores in preschool children [22].
3) Family-related factors
The family history was identified by four reviewed studies [11,23,29,30] and consanguinity was reported in three studies [19,25,26] as being significantly associated with DDs. The prevalence of DDs was significant among boys living in rural areas with scarce health and educational resources, in addition to low family income [22,28]. A study conducted in Egypt found an association between paternal education level and DDs in children [26]. Narrow spacing between children was also identified as a risk factor in a recent Saudi study [12].
DISCUSSION
In 2016, approximately 52.9 million children worldwide were reported to be experiencing DDs. Because the majority of the world's population lives in LMICs, DDs and abnormalities are more common in those countries [31]. According to the World Health Organization, 10% of the population in each country's population has a disability of one kind or another [32]. The current literature review indicates that the prevalence of DDs in the Arab world is lower (27.47%) than that reported in the Lancet Global Health 2016 study (43%), but higher than the global average (10%). According to the current literature analysis, the significant risk factors for higher rates of DDs in Arab populations include a lower level of maternal education, a history of pregnancy, birth, and perinatal complications, as well as the child's sex.
Our results showed that the DD prevalence varied both within and between countries. For instance, most studies that reported a high prevalence were carried out in LMICs, including Mauritania, Algeria, Iraq, Palestine, Jordan, and Lebanon, where low socio-economic status (SES) is common. The technique of performing developmental assessments varies among practitioners. In several studies, qualified professionals (i.e., nurses or physicians) measured development scores, but others stated that information on children's developmental status was obtained from their mothers or caregivers. Moreover, the heterogeneity of the findings may be explained by variations in lifestyles and SES among Arab countries, as well as between different geographic areas within countries. Geographic differences in DD prevalence have been previously reported [33,34].
Regarding maternal factors, research by Muller et al. [35] (2019) revealed that prenatal and perinatal complications and morbidities contribute to poor psychomotor development in children, which is consistent with the current review findings. In addition to maternal-related factors, a recent review pointed out that child-related factors such as sex, birth weight, premature birth, childhood illness, and injuries also influence child well-being and development, which are congruent with findings from Iran and South Asia, respectively [36,37]. A study conducted by Soleimani et al. [36] (2018) showed a higher prevalence of DDs in boys than in girls. Concerning birth weight, a systematic review concluded that most studies documented low birth weight as a risk factor for DDs [37].
Finally, family-related factors are relevant, such as the family's SES, which is reflected by a combination of indices including family income, parents' education and work status, family size, and residency. Researchers studying child development have paid special attention to family SES because it produces disparities among households in terms of home circumstances that promote children's well-being and development [33,34], which agrees with the current review results.
It is important to recognize a few limitations of our study. Even though we identified adequate research for this review, the distribution of studies across the Arab world was uneven, and the sample characteristics (such as sample size and age group) differed from one another. As a result, the overall findings may either over- or under-represent the DD burden in this area. Furthermore, some Arab countries were noticeably underrepresented, indicating the lack of high-quality prevalence data outside of the countries under study. Another notable limitation is the variation in case definitions and diag-nostic procedures used by researchers. Although the vast majority of research employed definitions based on the American Academy of Pediatrics Neurology guidelines, this study could not take into account all potential variations in the case description and diagnosis of DDs.
In the Arab world, DDs are prevalent among preschool children, although the rate varies among countries. Governments, legislators, and international organizations should think about bolstering global cooperation in DD screening and developing initiatives to assist in reducing the risks related to DDs. Local governments and policymakers ought to consider tightening rules to address social and environmental risk factors related to DDs in this population, as well as increasing public awareness about the early detection of children with delays, which would allow parents and caregivers to implement strategies to address problems before school entry. A combination of nurse- and patient-targeted educational interventions may also help to lessen the burden of DDs. The methods and standards used to assess and diagnose DDs in this population should be standardized.
In light of this review, additional studies are required to determine the prevalence of DD and its risk factors among Arab preschool children. This type of research is required to develop and implement primary preventive programs aimed at detecting and diagnosing DD children as early as possible. Research on this topic is also essential for the development of screening programs, which would entail low-cost preventive measures and public education campaigns to reduce the burden of disease in adulthood.
CONCLUSION
The prevalence of DDs in preschool children is substantially high in the Arab world (27.5%), which has implications for both national and international health. This analysis revealed that factors related to the child, the mother, and the family all contribute significantly to the risk of preschool children developing DD, with maternal factors such as prenatal and perinatal problems being the most common. In order to reduce the disease burden in adults, it is essential to identify and diagnose DDs and their associated risk factors as early as possible through screening programs.